NAPLEX
The questions in this section are intended to test your knowledge and skills in pharmacy practice including pharmacy calculations and biostatistics for pharmacy student pursuing to get license. Select all that applies. May have multiple answers.
Click on the right arrow to go to the next question. If the arrow is missing hover your mouse to the lower right, above the ad until the mouse is clickable.
NAPLEX | pharmaceutics / kinetics
Congratulations - you have completed NAPLEX | pharmaceutics / kinetics.
You scored %%SCORE%% out of %%TOTAL%%.
Your performance has been rated as %%RATING%%
Your answers are highlighted below.
Question 1 |
If a 75 Kg patient is given 1.5 gm of vancomycin what is the excepted maximum blood concentration (Cmax) if Vd of 0.9L/kg is used?
25.6 mg/L | |
22.2 mg/mL | |
15.3 mg/mL | |
26.1 mg/mL | |
9.5 mg/ml |
Question 1 Explanation:
C = Dose/Vd
C= 1500mg/67.5L = 22.2 mg/L
C= 1500mg/67.5L = 22.2 mg/L
Question 2 |
The bioavailability of Ciprofloxacin is 70%. If a patient is prescribed 400mg IV Q8H, what would be the closest available oral conversion? Oral Ciprofloxacin comes as 250mg, 500mg and 750 mg tablets?
250 mg TID | |
500 mg TID | |
750 mg TID | |
500mg BID | |
750mg BID |
Question 2 Explanation:
400 mg IV Q8H = 1200 mg daily
Difference between IV and PO bioavailability = 100% - 70% = 30 % =0.03 (we will need 30% more of PO drug to receive the same daily dose of Ciprofloxacin)
1200mg x 0.30 = 360mg
360mg + 1200mg = 1560 mg or 500 mg TID
Difference between IV and PO bioavailability = 100% - 70% = 30 % =0.03 (we will need 30% more of PO drug to receive the same daily dose of Ciprofloxacin)
1200mg x 0.30 = 360mg
360mg + 1200mg = 1560 mg or 500 mg TID
Question 3 |
Which of the following statements best describes piperacillin/tazobactam ’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 3 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 4 |
Which of the following statements best describes Levofloxacin’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 4 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 5 |
Administration of 25mg of a XYZ drug intravenously and 100mg XYZ drug orally revealed the same area under the curve. What is the bioavailability of the oral drug?
100% | |
75% | |
50% | |
25% |
Question 5 Explanation:
F = (AUC PO)/(AUC IV) x (Dose IV)/(Dose PO)
F = 1/1 x 25/100 = 0.25 X 100% = 25%
F = 1/1 x 25/100 = 0.25 X 100% = 25%
Question 6 |
Which of the following statements best describes Tigecycline’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 6 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, tigecycline, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, tigecycline, vancomycin.
Question 7 |
DP is 42 YOM admitted to the ER from an overdose of trazodone 20 100mg tablets 6 hours ago. ER physician wants to know how long will it take for DP’s trazodone to be eliminated from the body. The half-life of trazodone is 10hrs.
10 hours later | |
20 hours later | |
30 hours later | |
40 hours later | |
50 hours later |
Question 7 Explanation:
It takes 5 half lives for a drug to be theoretically completely eliminated (98% eliminated). 5 X 10 hours = 50 hours.
Question 8 |
Volume of Distribution of Levetiracetam is 0.7 L/kg, what would be the maximum blood concentration (Cmax) following infusion of a 1gm IVB on a patient that weighs 35kg.
32.4 mg/L | |
40.8 mg/L | |
37.2 mg/L | |
55.9 mg/L |
Question 8 Explanation:
Cmax = Dose/Vd
Cmax = 1000mg/24.5L = 40.8 mg/L
Cmax = 1000mg/24.5L = 40.8 mg/L
Question 9 |
If the Half-life of the Levetiracetam is 5 hrs, what is the expected blood Levetiracetam concentration after 12hrs? (Cmax = 40.8 mg/L)
6.2 mg/L | |
5.8 mg/L | |
6.8mg/L | |
7.1 mg/L | |
7.6 mg /L |
Question 9 Explanation:
Ke = 0.693/(t1/2 ) = 0.14 h-1
C = Cmax x e-ke x t = 40.8 x e-0.14 x 12 = 7.6 mg/L
C = Cmax x e-ke x t = 40.8 x e-0.14 x 12 = 7.6 mg/L
Question 10 |
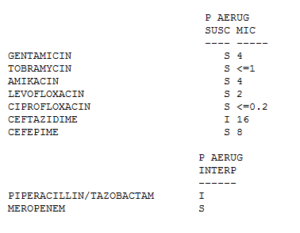
CL is a 44-year-old female admitted in hospital with UTI and C. Difficle infection. Her weight is 88 kg. She has a normal renal function. Patient is allergic to quinolones. She is currently on Cefepime 2gm IV every 12 hours, Metronidazole 500mg IV every 6 hours and Vancomycin PO 250mg four times daily. Two days later the blood culture was positive for Pseudomonas Aeruginosa with following sensitivity and MIC: The volume of distribution of Cefepime is 18 L. After a 30-minute infusion of Cefepime what is the drug blood concentration? Round to the nearest whole number.
111 mg/L | |
252 mg/L | |
193 mg/L | |
222 mg/L |
Question 10 Explanation:
C = Dose/Vd = 2000mg/18L
= 111 mg/L
= 111 mg/L
Question 11 |
CL is a 44-year-old female admitted in hospital with UTI and C. Difficle infection. Her weight is 88 kg. She has a normal renal function. Patient is allergic to quinolones. She is currently on Cefepime 2gm IV every 12 hours, Metronidazole 500mg IV every 6 hours and Vancomycin PO 250mg four times daily. Two days later the blood culture was positive for Pseudomonas Aeruginosa with following sensitivity and MIC: The elimination half-life of Cefepime is 2 hours. Approximately after how many half-lives would the cefepime blood concentration fall below MIC?
3 half life | |
2 half lives | |
4 half lives | |
5 half lives |
Question 11 Explanation:
k= 0.693/(t1/2 )= 0.345
Fraction remaining after 1 half life (2 hours) = e^(-kt)= e – 0.345 x 2= 0.50
Amount remaining after 1 half life (2 hours) = 0.50 x 111mg/mL = 55.5 mg/mL
Amount remaining after 2 half lives (4 hours) = 0.25 x 111 mg/mL = 27.75 mg/mL
Amount remaining after 3 half lives (6 hours) = 0.125 x 111 mg/mL = 13.875 mg/mL
Amount remaining after 4 half lives (8 hours) = 0.0625 x 111 mg/mL = 6.93 mg/mL
Since the MIC of Cefepime is 8, it will take 4 half lives for cefepime to reach a concentration of 6.93 mg/mL, which is a blood concentration below MIC.
Amount remaining after 1 half life (2 hours) = 0.50 x 111mg/mL = 55.5 mg/mL
Amount remaining after 2 half lives (4 hours) = 0.25 x 111 mg/mL = 27.75 mg/mL
Amount remaining after 3 half lives (6 hours) = 0.125 x 111 mg/mL = 13.875 mg/mL
Amount remaining after 4 half lives (8 hours) = 0.0625 x 111 mg/mL = 6.93 mg/mL
Since the MIC of Cefepime is 8, it will take 4 half lives for cefepime to reach a concentration of 6.93 mg/mL, which is a blood concentration below MIC.
Question 12 |
CL is a 44-year-old female admitted in hospital with UTI and C. Difficle infection. Her weight is 88 kg. She has a normal renal function. Patient is allergic to quinolones. She is currently on Cefepime 2gm IV every 12 hours, Metronidazole 500mg IV every 6 hours and Vancomycin PO 250mg four times daily. Two days later the blood culture was positive for Pseudomonas Aeruginosa with following sensitivity and MIC: 12. Approximately after how many hours would the Cefepime blood concentration fall below MIC?
2 hours | |
4 hours | |
6 hours | |
8 hours |
Question 12 Explanation:
It will take 4 half lives for cefepime to reach a concentration of 6.93 mg/mL Since the MIC of Cefepime is 8, it will take approximately 8 hours for cefepime to reach a concentration of 6.93 mg/mL, which is a blood concentration below MIC.
Question 13 |
What is the T>MIC achieved by Cefepime 1gm IV every 12 hours? Vd of cefepime is 18L, half life is 2 hours, and MIC = 8.
70.5% | |
53.6% | |
46.7% | |
68.2% |
Question 13 Explanation:
T>MIC = ln ( Dose/(Vd x MIC) ) x (t1/2)/ln〖(2)〗 x 100/DI
T>MIC = ln ( (1000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 46.7%
T>MIC = ln ( (1000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 46.7%
Question 14 |
The pharmacodynamic of cefepime is optimized if T>MIC is greater than 60-70%. What dose and frequency would attain this?
2 grams IV Q24H | |
1 grams IV Q8H | |
2 grams IV Q12H | |
2 grams IV Q18H |
Question 14 Explanation:
T>MIC = ln ( Dose/(Vd x MIC) ) x (t1/2)/ln〖(2)〗 x 100/DI
T>MIC = ln ( (2000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 63.3%
T>MIC = ln ( (2000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 63.3%
Question 15 |
What is the expected vancomycin serum concentration after a 3-day therapy of vancomycin 250mg oral four times daily? Round to the nearest whole number.
176 mg | |
186 mg | |
196 mg | |
Vancomycin is not absorbed when taken orally |
Question 15 Explanation:
Oral vancomycin is not absorbed or metabolized, rather it is excreted in the feces unchanged, making it a drug of choice for the treatment of C. difficile infections. Serum concentrations with oral vancomycin should not be measured.
Question 16 |
What pharmacodynamics property is demonstrated by Metronidazole?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: Cmax/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: AUC/MIC |
Question 16 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 17 |
HN is a 29-year-old female who is the hospital with a cellulitis. Physician would like pharmacy to dose the vancomycin. She weighs 67kg, height 70 feet, creatinine clearance 120 mL/min. Calculate the population specific half-life. Use Vd of 0.7L/kg
2.7 h | |
4.5 h | |
2.1 h | |
3.4 h |
Question 17 Explanation:
t1/2 = (0.693 x Vd)/CL
t1/2 = (0.693 x 700mL/kg x67kg)/(120mL/min)
= 270 minutes = 4.5 h
t1/2 = (0.693 x 700mL/kg x67kg)/(120mL/min)
= 270 minutes = 4.5 h
Question 18 |
HN is a 29-year-old female who is the hospital with a cellulitis. Physician would like pharmacy to dose the vancomycin. She weighs 67kg, height 70 feet, creatinine clearance 120 mL/min.
You decide to give vancomycin 1gm IV every 8 hours. Vancomycin trough was 24.5 prior to the 5th dose. Vancomycin was held. 5 hours later another vancomycin level was ordered it came back 14.5. Calculate the patient specific half-life. Round to the nearest whole number.
8 h | |
12 h | |
5 h | |
7 h |
Question 18 Explanation:
Ke= ln〖C1-lnC2 〗/(t2-t1)
Ke= ln〖(24.5)-ln〖(14.5)〗 〗/(37-32) = 0.104
T1/2= 0.693/0.104 = 6.66 h = 7h
Ke= ln〖(24.5)-ln〖(14.5)〗 〗/(37-32) = 0.104
T1/2= 0.693/0.104 = 6.66 h = 7h
Question 19 |
After administration of 50mg of a drug intravenously and 100mg of the same drug orally revealed same drug blood concentration. What is the bioavailability of the oral drug?
40 % | |
20 % | |
80 % | |
50 % |
Question 19 Explanation:
F = (AUC PO)/(AUC IV) x (Dose IV)/(Dose PO)
F = 1/1 x 50/100 = 0.5 X 100% = 50%
F = 1/1 x 50/100 = 0.5 X 100% = 50%
Question 20 |
HT is a 56-year-old man who is being treated with tobramycin and oxacillin for his cellulitis. HT’s weight is 76 kg, height is 6’ 2”, Creatinine clearance 128mls/hr. After a 500mg dose of tobramycin his 9hrs random came back at 6.5 mg/L and 14hrs 1.2mg/L. Calculate the half-life and elimination rate constant.
0.34 h-1, 2.1 h | |
0.67 h-1, 1.03 h | |
0.28 h-1, 2.47 h | |
0.56 h-1, 1.23 h |
Question 20 Explanation:
Ke= ln〖C1-lnC2 〗/(t2-t1)
Ke= ln〖(6.5 mg/L)-ln〖(1.2 mg/L)〗 〗/((14-9) ) = 0.34 h-1
T1/2= 0.693/0.34 = 2.1 h
Ke= ln〖(6.5 mg/L)-ln〖(1.2 mg/L)〗 〗/((14-9) ) = 0.34 h-1
T1/2= 0.693/0.34 = 2.1 h
Question 21 |
Which of the following is true?
Acidic drugs are highly protein bound therefore have high volume of distribution. | |
Acidic drugs are less protein bound therefore have low volume of distribution | |
Acidic drugs are highly protein bound therefore have low volume of distribution | |
Acidic drugs are less protein bound therefore have high volume of distribution |
Question 21 Explanation:
Acidic drugs are primarily bind to albumin (highly protein bound). Drugs that are highly protein/plasma bound tend to stay in the blood longer, resulting in a lower volume of distribution. Drugs that primarily distribute into tissue have a high volume of distribution.
Question 22 |
What pharmacodynamics property is demonstrated by azithromycin?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 22 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 23 |
What pharmacodynamics property is demonstrated by Tobramycin?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 24 |
Which of the following is true?
Basic drugs are highly protein bound therefore have high volume of distribution. | |
Basic drugs are less protein bound therefore have low volume of distribution. | |
Basic drugs are highly protein bound therefore have low volume of distribution. | |
Basic drugs are less protein bound therefore have high volume of distribution. |
Question 24 Explanation:
Basic drugs are less protein bound and therefore readily distribute into tissue, resulting in a higher volume of distribution. These drugs often stay for longer periods of time in organs and tissues, often leading to higher concentrations, narrower therapeutic index and decreased clearance.
Question 25 |
SR is a 72 year old female admitted to ICU with PNA, A Fib, CHF with preserved left ventricular function. She weighs 76 kg. She has history of lung cancer for which she is being treated with cyberknife and chemotherapy as outpatient, history of hypertension, hyperlipidemia, hypothyroidism, COPD. On admission her WBC is 1.0 K/uL, bands of 32% and segs of 42%. SR was started on Vancomycin, Levofloxacin and Aztreonam for HAP. She is also on the electrolyte replacement protocol. She is allergic to PCN/cephalosporin (rash). For her A. Fib she was given Amiodarone 400mg orally BID and Diltiazem 10mg/hr. She also received few doses of furosemide for her CHF. What significant drug / drug interaction do you identify?
Furosemide and Amiodarone | |
Vancomycin and Amiodarone | |
Aztreonam and Amiodarone | |
Levofloxacin and Amiodarone |
Question 25 Explanation:
There is a drug interaction between levofloxacin and amiodarone, which may increase the risk of QT prolongation. Levofloxacin is associated with QT prolongation and rarely torsades de pointes. Amiodarone also has a risk of QT prolongation and torsades de pointes. This drug interaction is possible for days to weeks after amiodarone is discontinued because amiodarone has a long half-life. There is also a drug interaction with furosemide and amiodarone. Caution must be used because loop diuretics can lower potassium and magnesium levels, which can cause amiodarone to not work effectively, but patient is on electrolyte replacement protocol and on it for short duration.
Reference:
Gold Standard, Inc. Levofloxacin. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=746&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Once you are finished, click the button below. Any items you have not completed will be marked incorrect.
There are 25 questions to complete.
|
List |

Comments are closed.