BCPS
- Cardiovascular
- Endocrine
- Gastrointestinal disorder
- Infectious disease
- Men’s and women’s health
- Neurology
- Oncology
- Ophthalmic and otics
- Pain management
- Psychiatric
- Renal disease / fluids & electrolytes
- Respiratory
- Skin conditions
- Special populations
- Pharmacokinetics pharmacodynamics
- Biostatistics and pharmacoeconomics
- Pharmacy policy, procedure and regulations
The questions in this section are intended to test your knowledge and skills on pharmacotherapy including biostatistics for practicing pharmacists and pharmacist preparing for BCPS (Board Certified Pharmacotherapy Specialist)
Click on the right arrow to go to the next question. If the arrow is missing hover your mouse to the lower right, above the ad until the mouse is clickable.
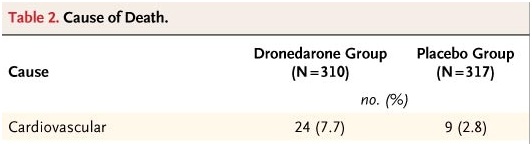 Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure.
Given the data above what is the absolute risk of cardiovascular death with Dronedarone group in severe heart failure patients?
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure.
Given the data above what is the absolute risk of cardiovascular death with Dronedarone group in severe heart failure patients?
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure.
What is the relative risk of cardiovascular death using Dronedarone therapy compared to placebo?
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure
What is the absolute risk of cardiovascular death in placebo group in severe heart failure patients?
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure
What is the relative risk increase using Dronedarone compared to placebo in severe heart failure patients?
BCPS Practice Questions
Congratulations - you have completed BCPS Practice Questions.
You scored %%SCORE%% out of %%TOTAL%%.
Your performance has been rated as %%RATING%%
Your answers are highlighted below.
Question 1 |
Patients with HLA-B* 1502 are increased risk of Steven-Johnson syndrome from what Anti-epileptic medication?
Carbamazepine
| |
Gabapentin | |
Valproic acid
| |
Levetiracetam
|
Question 1 Explanation:
There is a strong relationship between HLA-B*1502 and carbamazepine-induced SJS and TEN in Han-Chinese, Thai, and Malaysian populations.1 This same relationship and between HLA*1502 and SJS/TEN has been also found with phenytoin and lamotrigine.
Reference:
Tangamornsuksan, W, Chaiyakunapruk, N, et al. Relationship between the HLA-B*1502 allele and carbamazepine-induced stevens-johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2013;149(9):1025-1032. doi:10.1001/jamadermatol.2013.4114.
Reference:
Tangamornsuksan, W, Chaiyakunapruk, N, et al. Relationship between the HLA-B*1502 allele and carbamazepine-induced stevens-johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2013;149(9):1025-1032. doi:10.1001/jamadermatol.2013.4114.
Question 2 |
FM is a 49 year old female admitted to the ER with diagnosis of DKA, due to her poor respiratory status she is intubated. Pertinent labs are: Na 128 mmol/L, K 7.6 mmol/L, Cl 98 mmol/L, CO2 6 mmol/L, SCr 3.4 mg/dL, BG 1813 mg/dL, pH 6.84, pCO2 27.2 mmHg.
What is FM’s Anion gap?
2 | |
42 | |
24 | |
13 |
Question 2 Explanation:
Na - (Cl- + HCO3)= 128 mmol/L - (98 mmol/L + 6 mmol/L)
= 128 --104 = 24
Use laboratory sodium to calculate anion gap, not the corrected sodium.
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
= 128 --104 = 24
Use laboratory sodium to calculate anion gap, not the corrected sodium.
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Question 3 |
FM is a 49 year old female admitted to the ER with diagnosis of DKA, due to her poor respiratory status she is intubated. Pertinent labs are: Na 128 mmol/L, K 7.6 mmol/L, Cl 98 mmol/L, CO2 6 mmol/L, SCr 3.4 mg/dL, BG 1813 mg/dL, pH 6.84, pCO2 27.2 mmHg.
What is the appropriate choice of intravenous fluid (IVF) to initiate on FM at this time?
NS | |
D5NS | |
NS with 150meq of NaHCO3 | |
Sterile Water with 150meq of NaHCO3 |
Question 3 Explanation:
Her corrected sodium is high,her glucose is high so she should not receive NS or any IVF with D5W. Her pH is <6.9 so she must receive NaHCO3. pH less than 6.9 is an indication for a bicarb drip. She should not receive NS with NaHCO3, makes the solution hypertonic.
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Question 4 |
FM is a 49 year old female admitted to the ER with diagnosis of DKA, due to her poor respiratory status she is intubated. Pertinent labs are: Na 128 mmol/L, K 7.6 mmol/L, Cl 98 mmol/L, CO2 6 mmol/L, SCr 3.4 mg/dL, BG 1813 mg/dL, pH 6.84, pCO2 27.2 mmHg.
What is the appropriate treatment of choice for FM’s hyperkalemia at this time?
Sodium polystyrene 60gm PR x1 | |
Albuterol 10mg via neb | |
Continue the Insulin drip no other treatment needed | |
Sodium polystyrene 60gm PR x1 and Albuterol 10mg via neb |
Question 4 Explanation:
Current potassium level is 7.6mmol/L. She is currently receiving Insulin, which is a treatment for hyperkalemia. Because the pH is below 6.9, she should receive Sodium bicarbonate, which pushes potassium intracellularly in response to a rise in systemic pH, this will also bring her potassium down.
Reference:
Treatment and prevention of hyperkalemia in adults. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/treatment-and-prevention-of-hyperkalemia-in-adults. Accessed May 16, 2016.
Reference:
Treatment and prevention of hyperkalemia in adults. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/treatment-and-prevention-of-hyperkalemia-in-adults. Accessed May 16, 2016.
Question 5 |
In a publication, observed mean weight of 200 patients was reported as 69.4 ±9.3 kg. If 9.3 kg is the SEM (standared error of mean), calculate the SD (standared deviation) and variance?
131.52kg/17298kg | |
78.7kg/9.3kg | |
87.24kg/69.4kg | |
69.4kg/131kg |
Question 5 Explanation:
SEM x √n = SD
9.3 x √200 = 131.52 kg = SD
SD2 (square) = variance
131.522 = 17298 kg = variance
Reference:
Statistics at Square One The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
9.3 x √200 = 131.52 kg = SD
SD2 (square) = variance
131.522 = 17298 kg = variance
Reference:
Statistics at Square One The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 6 |
FM was transferred to ICU on Propofol, Norepinephrine drip, D5W with 150meq of NaHCO3 at 150mls/hr, Insulin drip, Potassium, Magnesium and Phosphorus replacement protocol. Few hours later, labs were repeated and pertinent labs are: Na 146 mmol/L, K 2.5 mmol/L, Cl 103 mmol/L, CO2 20 mmol/L, Phosphorus 1.2 mg/dL, triglycerides 741 MG/Dl, Blood Glucose 735 mg/dL. ABG: pH 7.265, pCO2 40.2 mmHg, pO2 82 mmHg. Serum Creatinine 1.2 mg/dl.
What should be FM’s appropriate drug of choice for sedation?
Propofol | |
Midazolam | |
Fentanyl | |
Cisatracurium Besylate |
Question 6 Explanation:
Because this patient has high triglycerides, Propofol should be avoided for sedation since it has been shown to increase triglycerides. A better alternative is midazolam. Fentanyl should not be used monotherapy. CisatracuriumBesylate is a paralytic.
Reference:
Gold Standard, Inc. Sodium Chloride. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=1554&sec=monindi&t=0. Accessed: May 16, 2016.
Reference:
Gold Standard, Inc. Sodium Chloride. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=1554&sec=monindi&t=0. Accessed: May 16, 2016.
Question 7 |
FM was transferred to ICU on Propofol, Norepinephrine drip, D5W with 150meq of NaHCO3 at 150mls/hr, Insulin drip, Potassium, Magnesium and Phosphorus replacement protocol. Few hours later, labs were repeated and pertinent labs are: Na 146 mmol/L, K 2.5 mmol/L, Cl 103 mmol/L, CO2 20 mmol/L, Phosphorus 1.2 mg/dL, triglycerides 741 MG/Dl, Blood Glucose 735 mg/dL. ABG: pH 7.265, pCO2 40.2 mmHg, pO2 82 mmHg. Serum Creatinine 1.2 mg/dl.
What should be FM’s drug of choice for treatment of chronic high triglycerides?
Fish oil | |
Fenofibrate | |
Atorvastatin | |
Treatment not needed until triglycerides >1000 mg/dl |
Question 7 Explanation:
For triglyceride levels above 500 mg/dL, it is reasonable to start pharmacological therapy in addition to lifestyle therapy. Fibrates are most effective in decreasing triglyceride levels. Fish oil and Atorvastatin not the best drug for lowering triglycerides. Statins are first line agent to reduce LDL.
Reference:
Stone NJ, Robinson J, Liechtenstein HA, et al. 2013 ACC/AHA guidelines on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. Available at http://circ.ahajournals.org/content/ early/2013/11/11/01.cir.0000437738.63853.7a. Accessed May 4, 2014
Reference:
Stone NJ, Robinson J, Liechtenstein HA, et al. 2013 ACC/AHA guidelines on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. Available at http://circ.ahajournals.org/content/ early/2013/11/11/01.cir.0000437738.63853.7a. Accessed May 4, 2014
Question 8 |
FM was transferred to ICU on Propofol, Norepinephrine drip, D5W with 150meq of NaHCO3 at 150mls/hr, Insulin drip, Potassium, Magnesium and Phosphorus replacement protocol. Few hours later, labs were repeated and pertinent labs are: Na 146 mmol/L, K 2.5 mmol/L, Cl 103 mmol/L, CO2 20 mmol/L, Phosphorus 1.2 mg/dL, triglycerides 741 MG/Dl, Blood Glucose 735 mg/dL. ABG: pH 7.265, pCO2 40.2 mmHg, pO2 82 mmHg. Serum Creatinine 1.2 mg/dl.
Which of the following is appropriate course of action for FM in regards to her low phosphate level?
Give 30mmoles of K Phosphate for phosphate level 1.2mg/dl | |
Give 30mmoles of Na Phosphate for phosphate level 1.2mg/dl | |
It is not recommended to replace phosphate unless concentration falls below 1.0 mg/dl | |
Replacing phosphate can cause hypermagnesemia and hypercalcemia |
Question 8 Explanation:
The current phosphate is 1.2 mg/dL. It is not recommended to replace phosphate unless concentrations fall below 1.0 mg/dL. When phosphate is replaced for level greater than 1.0mg/dlthere is actually a risk of adverse effects such as hypomagnesemia or hypocalcemia.
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodatecom. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults-treatment?. Accessed May 16, 2016
Reference:
Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodatecom. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults-treatment?. Accessed May 16, 2016
Question 9 |
FM was transferred to ICU on Propofol, Norepinephrine drip, D5W with 150meq of NaHCO3 at 150mls/hr, Insulin drip, Potassium, Magnesium and Phosphorus replacement protocol. Few hours later, labs were repeated and pertinent labs are: Na 146 mmol/L, K 2.5 mmol/L, Cl 103 mmol/L, CO2 20 mmol/L, Phosphorus 1.2 mg/dL, triglycerides 741 MG/Dl, Blood Glucose 735 mg/dL. ABG: pH 7.265, pCO2 40.2 mmHg, pO2 82 mmHg. Serum Creatinine 1.2 mg/dl.
What should the IVF be changed to?
½ NS | |
NS | |
D5NS | |
Keep the NaHCO3 |
Question 9 Explanation:
For sodium level above 145 mmol/L, the IVF should be ½ NS. For sodium level below 145 mmol/L the IVF should be NS. The corrected sodium indicates a level that is still above 145 mmol/L. Bicarbonate drip should be discontinued once pH>6.9. Dextrose should not be given for blood glucose >200 mg/dl.
Reference:
I. Kitabchi A, Umpierrez G, Miles J, et al. Hypergly¬cemic crises in adult patients with diabetes. Diabe¬tes Care 2009;32:1335-43
II. Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Reference:
I. Kitabchi A, Umpierrez G, Miles J, et al. Hypergly¬cemic crises in adult patients with diabetes. Diabe¬tes Care 2009;32:1335-43
II. Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Question 10 |
FM was transferred to ICU on Propofol, Norepinephrine drip, D5W with 150meq of NaHCO3 at 150mls/hr, Insulin drip, Potassium, Magnesium and Phosphorus replacement protocol. Few hours later, labs were repeated and pertinent labs are: Na 146 mmol/L, K 2.5 mmol/L, Cl 103 mmol/L, CO2 20 mmol/L, Phosphorus 1.2 mg/dL, triglycerides 741 MG/Dl, Blood Glucose 735 mg/dL. ABG: pH 7.265, pCO2 40.2 mmHg, pO2 82 mmHg. Serum Creatinine 1.2 mg/dl.
When should FM’s insulin drip be discontinued and switched to subcutaneous insulin?
Once BG <200 mg/dl and Serum Bicarbonate>25 meq/L | |
Once BG <200 mg/dl and Venous pH >7.4 | |
Once BG< 150 mg/dl and Serum Bicarbonate>25 meq/L | |
Once BG<200 mg dl and Anion gap <= 12 |
Question 10 Explanation:
Insulin drip can be discontinued once BG<200mg/dl AND Anion gap less than or equal to 12 OR BG< 200mg/dl and Venous pH is >7.3 and Serum Bicarb is 15 meq/L or more.
Reference:
I. Kitabchi A, Umpierrez G, Miles J, et al. Hypergly¬cemic crises in adult patients with diabetes. Diabe¬tes Care 2009;32:1335-43
II. Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Reference:
I. Kitabchi A, Umpierrez G, Miles J, et al. Hypergly¬cemic crises in adult patients with diabetes. Diabe¬tes Care 2009;32:1335-43
II. Diabetic ketoacidosis and hyperosmolar hyperglycemic state in adults: Treatment. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/diabetic-ketoacidosis-and-hyperosmolar-hyperglycemic-state-in-adults. Accessed May 16, 2016.
Question 11 |
Which of the following is/are nominal data?
Sex | |
Race | |
Blood group | |
A, B and C. |
Question 11 Explanation:
Nominal data is considered unordered categories. Sex answers fall into male or female which is unordered. Race can be multiple answers such as Caucasian, African American, Asian, etc which is unordered. Blood group can only have blood type O, A, B, or AB which is also unordered. Ordered, or ordinal data would have categories that are in some sort of order.
Reference:
I. "Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Reference:
I. "Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 12 |
SR is a 72 year old female admitted in ICU with pneumonia, A. Fib, CHF with preserved left ventricular function. She weighs 76 kg. She has history of lung cancer for which she is being treated with cyberknife and chemotherapy as outpatient, history of hypertension, hyperlipidemia, hypothyroidism, COPD. On admission her WBC is 1.0 K/uL, bands of 32% and segs of 42%. SR was started on Vancomycin, Levofloxacin and Aztreonam for hospital acquired pneumonia (HAP). She is also on the electrolyte replacement protocol. She is allergic to PCN/cephalosporin (rash). For her A. Fib she was given Amiodarone 400mg orally BID and Diltiazem 10mg/hr. She also received few doses of furosemide for her CHF.
What is SR’s absolue neutrophil count(ANC)?
740 | |
500 | |
420 | |
320 |
Question 12 Explanation:
WBC * ((Segs/100) + (Bands/100)) =ANC = 1.0 k/uLx (0.32 + 0.42) = 740
Reference:
Whalen KL, Borja-Hart N (2015). Interpretation of Clinical Laboratory Data. In: Nemire RE, Kier KL, Assa-Eley M. Nemire R.E., Kier K.L., Assa-Eley M Eds. Ruth E. Nemire, et al.eds. Pharmacy Student Survival Guide, 3e. New York, NY: McGraw-Hill; 2015.
Reference:
Whalen KL, Borja-Hart N (2015). Interpretation of Clinical Laboratory Data. In: Nemire RE, Kier KL, Assa-Eley M. Nemire R.E., Kier K.L., Assa-Eley M Eds. Ruth E. Nemire, et al.eds. Pharmacy Student Survival Guide, 3e. New York, NY: McGraw-Hill; 2015.
Question 13 |
SR is a 72 year old female admitted in ICU with PNA, A Fib, CHF with preserved left ventricular function. She weighs 76 kg. She has history of lung cancer for which she is being treated with cyberknife and chemotherapy as outpatient, history of hypertension, hyperlipidemia, hypothyroidism, COPD. On admission her WBC is 1.0 K/uL, bands of 32% and segs of 42%. SR was started on Vancomycin, Levofloxacin and Aztreonamfor HAP. She is also on the electrolyte replacement protocol. She is allergic to PCN/cephalosporin (rash). For her A. Fib she was given Amiodarone 400mg orally BID and Diltiazem 10mg/hr. She also received few doses of furosemide for her CHF.
Physician would like to treat SR’s low ANC. Which of the following would be the treatment of choice with dose for her low ANC?
Filgrastim 380 mcg subcutaneously daily | |
Filgrastim 480 mcg subcutaneously daily | |
Erythropoietin 10,000 untis subcutaneously daily | |
Fresh Frozen Plasma (FFP) 15 mls/kg |
Question 13 Explanation:
Considering this patient had received chemotherapy (unable to determine when exactly), this dosage is consistent with the indication of primary prophylaxis in patients with nonmyeloid malignancies (5 mcg/kg/day subcutaneously).Erythropoietin is indicated for treatment of Anemia due to various causes. FFP is given in certain bleeding disorder to replace factors.
Reference:
Gold Standard, Inc. Filgrastim, G-CS. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=246&sec=monindi&t=0 Accessed: May 16, 2016.
Reference:
Gold Standard, Inc. Filgrastim, G-CS. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=246&sec=monindi&t=0 Accessed: May 16, 2016.
Question 14 |
SR is a 72 year old female admitted in ICU with PNA, A Fib, CHF with preserved left ventricular function. She weighs 76 kg. She has history of lung cancer for which she is being treated with cyberknife and chemotherapy as outpatient, history of hypertension, hyperlipidemia, hypothyroidism, COPD. On admission her WBC is 1.0 K/uL, bands of 32% and segs of 42%. SR was started on Vancomycin, Levofloxacin and Aztreonamfor HAP. She is also on the electrolyte replacement protocol. She is allergic to PCN/cephalosporin (rash). For her A. Fib she was given Amiodarone 400mg orally BID and Diltiazem 10mg/hr. She also received few doses of furosemide for her CHF.
What significant drug / drug interaction do you identify?
Furosemide and Amiodarone | |
Vancomycin and Amiodarone | |
Aztreonam and Amiodarone | |
Levofloxacin and Amiodarone |
Question 14 Explanation:
There is a drug interaction between levofloxacin and amiodarone, which may increase the risk of QT prolongation. Levofloxacin is associated with QT prolongation and rarely torsades de pointes. Amiodarone also has a risk of QT prolongation and torsades de pointes. This drug interaction is possible for days to weeks after amiodarone is discontinued because amiodarone has a long half-life. There is also a drug interaction with furosemide and amiodarone. Caution must be used because loop diuretics can lower potassium and magnesium levels, which can cause amiodarone to not work effectively, but patient is on electrolyte replacement protocol and on it for short duration.
Reference:
Gold Standard, Inc. Levofloxacin. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=746&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Reference:
Gold Standard, Inc. Levofloxacin. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=746&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at:https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Question 15 |
SR’s TSH 0.041mIUn/ml (normal 0.36-3.74), she has been taking 125mcg of levothyroxine orally for more than a year. What would be the most appropriate drug regimen modification?
Increase dose of Levothyroxine to 150mcg oral daily | |
Decrease dose of levothyroxine to 100mcg oral daily | |
Increase dose of Levothyroxine to 150mcg IV daily | |
Decrease dose of levothyroxine to 100mcg IV daily |
Question 15 Explanation:
Decrease the dose to 100mcg orally daily. The TSH level is below therapeutic range (0.358--3.740 uIUn/mL). The TSH level is generally inversely related to the thyroid hormones’ levels. Bioequivalent of oral to intravenous levothyroxine is 2:1 ratio, so changing any dose to IV above 75mcg dose wound be to increase the dose.
Reference:
I. Bahn R, et al. hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the american thyroid association and american association of clinical endocrinologists. EndocrPract. 2011;17(3). Available at: https://www.aace.com/files/hyper-guidelines-2011.pdf. Accessed May 18, 2016.
Reference:
I. Bahn R, et al. hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the american thyroid association and american association of clinical endocrinologists. EndocrPract. 2011;17(3). Available at: https://www.aace.com/files/hyper-guidelines-2011.pdf. Accessed May 18, 2016.
Question 16 |
The mean decrease in Heart Rate after initiating a beta blocker XYZ in 90 patients was 24 beat per minute with standard error of 3.78 beats for minute. What would be the 95% confidence interval for the decrease in HR after initiating drug XYZ?
16.64-31.4mmHg | |
20.22-27.78mmHg | |
14.55-33.45mmHg | |
22.28-26.28 mmHg |
Question 16 Explanation:
24 + (1.96 x 3.78) = 31.4 mmHg
24 - (1.96 x 3.78) = 16.6 mmHg
The 95% confidence interval is from 16.6 mmHg to 31.4 mmHg, which means we can be 95% sure that the mean decrease in HR after starting beta blocker XYZ of the population falls within this range. You can also say that there is a 5% chance that the mean decrease in HR of the population falls outside of this range.
Reference:
I. "Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
24 - (1.96 x 3.78) = 16.6 mmHg
The 95% confidence interval is from 16.6 mmHg to 31.4 mmHg, which means we can be 95% sure that the mean decrease in HR after starting beta blocker XYZ of the population falls within this range. You can also say that there is a 5% chance that the mean decrease in HR of the population falls outside of this range.
Reference:
I. "Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 17 |
KC is a 84 year old female, comes in the ER from nursing home with SOB. Past medical history of COPD DM, Schizophrenia, HTN. Chest x-ray upon admission showed pneumonic infiltrate in the left lower lung and possible early pneumonia in the right lung base. WBC 15,300 /mm3,Temp 102 F, HR 103 beats per minute, BP 134/65 mmHg, RR 40 breaths per minute. She was not on any antibiotics prior to admission. Her nursing home meds include, Albuterol/Atrovent nebs, Amlodipine, Metformin, Risperidone, Glimepiride, Losartan and Prednisone.
Which of the following would be the appropriate antibiotics to treat KC’s pneumonia?
Levofloxacin and Ceftriaxone | |
Levofloxacin and Piperacillin/Tazobactam | |
Piperacillin/Tazobactam, Cefepime, Vancomycin | |
Levofloxacin, Piperacillin/Tazobactam, and Vancomycin. |
Question 17 Explanation:
A and B are incorrect because there is no MRSA coverage, and this patient has risk of MDR because she came from a nursing home. C is incorrect because Piperacillin/Tazobactam andcefepime provide duplicate coverage for pseudomonas. D is the correct answer because she came from a nursing home she should be treated as having healthcare-care associated pneumonia risk for MDR. She should be started on IV empiric therapy with Levofloxacin, Vancomycin, and Piperacillin/Tazobactam.
Reference:
Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J RespirCrit Care Med. 2005;171(4):388-416. doi:10.1164/rccm.200405-644st
Reference:
Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J RespirCrit Care Med. 2005;171(4):388-416. doi:10.1164/rccm.200405-644st
Question 18 |
If it was a community acquired pneumonia transferred to ICU what would be the antibiotics of choice considering the patient has no penicillin allergy and no pseudomonas risks?
Levofloxacin and Ceftriaxone | |
Levofloxacin and Vancomycin | |
Azithromycin, Vancomycin | |
Levofloxacin, Piperacillin/Tazobactam, and Vancomycin. |
Question 18 Explanation:
A is the correct answer because according to the IDSA CAP guidelines, antibiotics that should be started are a beta-lactam and either azithromycin or a fluoroquinolone for patients without penicillin allergy. For pseudomonas infections, empiric therapy can be with Piperacillin/Tazobactam plus levofloxacin or ciprofloxacin. B is wrong because this option does not include a beta-lactam. C and D are wrong because Piperacillin/Tazobactam is for pseudomonas infections. Vancomycin is inappropriate because this is community-acquired pneumonia and therefore the patient is not at risk for MRSA as he would be if he had healthcare or hospital acquired pneumonia.
Reference:
Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
Reference:
Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
Question 19 |
In a cohort study where the investigators looked at the association between smoking and throat cancer for 20 years found the relative risk of 14. How can this data best be interpreted?
14% of the throat cancers are due to smoking
| |
Smokers had 14% increased risk of throat cancer compared to non-smokers
| |
Smokers had 14 times the risk of throat cancer compared to non-smokers
| |
Smokers had 86% increased risk of throat cancer compared to non-smoker
|
Question 19 Explanation:
Relative risk is a proportion so when interpreting relative risk one can say “times as,” in this case it is 14 times the risk or is 14 times as likely.
Reference:
Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/
Reference:
Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/
Question 20 |
What is/are the risk factors for Pseudomonal Pneumonia ?
On mechanical ventilator for days | |
10 years history COPD | |
Chronic steroid use | |
All of the Above |
Question 20 Explanation:
The IDSA guidelines for CAP PNA list risk factors specific for pseudomonas which are alcoholism, structural lung diseases, such as bronchiectasis, or repeated exacerbations of severe COPD leading to frequent steroid and/or antibiotic use, On mechanical ventilator for >3 days, as well as prior antibiotic therapy.
Reference:
I. Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
II. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J RespirCrit Care Med. 2005;171(4):388-416. doi:10.1164/rccm.200405-644st.
Reference:
I. Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
II. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am J RespirCrit Care Med. 2005;171(4):388-416. doi:10.1164/rccm.200405-644st.
Question 21 |
What is/are the risk factor for MRSA pneumonia ?
Prior exposer to Ciprofloxacin and Levofloxacin | |
Recent influenza infection | |
ESRD | |
All of Above |
Question 21 Explanation:
The IDSA guidelines for CAP PNA list risk factors specific for MRSA, which are end-stage renal disease, injection drug abuse, prior influenza, and prior antibiotic therapy, especially
with fluoroquinolones. Infection with the influenza virus has been shown to be a risk factor for MRSA. Other risk factors for multi-drug resistant HAP, VAP, and HCAP are previous use of antibiotics within the last 90 days, current hospitalization of 5 d or more, local high occurrence antibiotic resistance, immunosuppressive state, or risk factors for HCAP (2 or more days of hospitalization in past 30 days, residence in a long term care facility or nursing home, family member with multidrug-resistant pathogen, home wound care, family member with multidrug-resistant pathogen, chronic dialysis within the last 30 days, or home infusion therapy). Investigations have shown that fluoroquinolones are associated with predisposing patients to MRSA infections. Several case control study demonstrated that exposure to either levofloxacin or ciprofloxacin use was associated with MRSA infection but not MSSA.
Reference:
I. Weber SG, Gold HS, Hooper DC, Karchmer AW, Carmeli Y. Fluoroquinolones and the Risk for Methicillin-resistant Staphylococcus aureus in Hospitalized Patients. Emerging Infectious Diseases. 2003;9(11):1415-1422. doi:10.3201/eid0911.030284
II. Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
Reference:
I. Weber SG, Gold HS, Hooper DC, Karchmer AW, Carmeli Y. Fluoroquinolones and the Risk for Methicillin-resistant Staphylococcus aureus in Hospitalized Patients. Emerging Infectious Diseases. 2003;9(11):1415-1422. doi:10.3201/eid0911.030284
II. Mandell L, Wunderink R, Anzueto A et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clinical Infectious Diseases. 2007;44(Supplement 2):S27-S72. doi:10.1086/511159.
Question 22 |
JP is a 40yr old male who was found lying on the floor with several empty liquor bottles by his friend. After being brought to the ER his serum alcohol level was found to be 475 mg/dl. Toxicology report negative except for high alcohol level. 2 hours after admission in the ER he was intubated and then transferred to ICU . His liver enzymes and renal function are normal. PT/INR within normal limit. No past medical history. Upon transfer medications includes Propofol, MVI daily, Lorazepam prn and Piperacillin/Tazobactam.
What measures can one take to prevent ventilator associated Pneumonia (VAP)?
Twice daily oral decontamination with Chlorhexidine | |
Give Pipercillin/Tazobactam 3.375gm IV q6hr prophylaxis | |
Elevate the head of the bed by 30-45 | |
A and C are appropriate measures to prevent VAP |
Question 22 Explanation:
The following 5 elements are part of the Institute of Healthcare Improvement VAP bundle: oral care with Chlorhexidine, head of bed elevation, DVT prophylaxis, SUP, and daily sedation assessment and spontaneous breathing trials. Other suggested measures for VAP prophylaxis are small bowel feeding instead of gastric feeding, prophylactic probiotics, alcohol based hand washing policy, early discontinuation of invasive devices, early tracheostomy, and reducing reintubation rates. Giving prophylaxis antibiotic is not recommended.
Reference:
Kalanuria AA, Zai W, Mirski M. Ventilator-associated pneumonia in the ICU. Critical Care. 2014;18(2):208. doi:10.1186/cc13775.
Reference:
Kalanuria AA, Zai W, Mirski M. Ventilator-associated pneumonia in the ICU. Critical Care. 2014;18(2):208. doi:10.1186/cc13775.
Question 23 |
JP is a 40yr old male who was found lying on the floor with several empty liquor bottles by his friend. After being brought to the ER his serum alcohol level was found to be 475 mg/dl. Toxicology report negative except for high alcohol level. 2 hours after admission in the ER he was intubated and then transferred to ICU . His liver enzymes and renal function are normal. PT/INR within normal limit. No past medical history. Upon transfer medications includes Propofol, MVI daily, Lorazepam prn and Piperacillin/Tazobactam.
What vitamin should the patient receive to avoid Wernicke- Korsakoff syndrome?
Thiamine | |
Cyanocobalamin | |
Magnesium | |
Folic Acid |
Question 23 Explanation:
Thiamine should be administered to prevent Wernicke’s encephalopathy.
Reference:
Management of moderate and severe alcohol withdrawal syndromes. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/management-of-moderate-and-severe-alcohol-withdrawal-syndromes. Accessed May 24, 2016.
Reference:
Management of moderate and severe alcohol withdrawal syndromes. Uptodate.com. 2016. Available at: http://www.uptodate.com/contents/management-of-moderate-and-severe-alcohol-withdrawal-syndromes. Accessed May 24, 2016.
Question 24 |
JP is a 40yr old male who was found lying on the floor with several empty liquor bottles by his friend. After being brought to the ER his serum alcohol level was found to be 475 mg/dl. Toxicology report negative except for high alcohol level. 2 hours after admission in the ER he was intubated and then transferred to ICU . His liver enzymes and renal function are normal. PT/INR within normal limit. No past medical history. Upon transfer medications includes Propofol, MVI daily, Lorazepam prn and Piperacillin/Tazobactam.
What is the treatment of choice for his acute alcohol withdrawal?
Haloperidol | |
Lorazepam | |
Ziprasidone | |
Alprazolam |
Question 24 Explanation:
Benzodiazepines are the most studied drugs for alcohol withdrawal treatment. Long-acting agents such as Diazepam and Chlordiazepoxide may be used. Antipsychotics are not recommended to treat alcohol withdrawal. Haloperidol is an antipsychotic, an inappropriate choice.
Reference:
Kosten T, O’Connor P. Management of drug and alcohol withdrawal. N Engl J Med 2003;348:1786- 95. A good general review of the management of the most common syndromes.
Management of moderate and severe alcohol withdrawal syndromes. Uptodatecom. 2016. Available at: http://www.uptodate.com/contents/management-of-moderate-and-severe-alcohol-withdrawal-syndromes. Accessed May 24, 2016
Reference:
Kosten T, O’Connor P. Management of drug and alcohol withdrawal. N Engl J Med 2003;348:1786- 95. A good general review of the management of the most common syndromes.
Management of moderate and severe alcohol withdrawal syndromes. Uptodatecom. 2016. Available at: http://www.uptodate.com/contents/management-of-moderate-and-severe-alcohol-withdrawal-syndromes. Accessed May 24, 2016
Question 25 |
JP is a 40yr old male who was found lying on the floor with several empty liquor bottles by his friend. After being brought to the ER his serum alcohol level was found to be 475 mg/dl. Toxicology report negative except for high alcohol level. 2 hours after admission in the ER he was intubated and then transferred to ICU . His liver enzymes and renal function are normal. PT/INR within normal limit. No past medical history. Upon transfer medications includes Propofol, MVI daily, Lorazepam prn and Piperacillin/Tazobactam.
Which of the following would be appropriate chronic treatment of choice for his alcohol withdrawal?
Acamprosate | |
Metronidazole | |
Diazepam | |
Duloxetine |
Question 25 Explanation:
Acamprosate is indicated for ethanol dependence, but only in patients who have become abstinent. Diazepam is not indicated for ethanol dependence but for acute alcohol withdrawal. Metronidazole may interfere with the metabolism of ethanol, resulting in disulfiram-like effects. Patients should try to avoid ethanol ingestion to avoid the risk of undesirable side effects. Duloxetine is not indicated to treat alcohol withdrawal.
Reference:
Doering P, Boothby L. Substance-related disorders: overview and depressants, stimulants, and hallucinogens. In: DiPiro J, Talbert R, Yee G, et al., eds. Pharmacotherapy. A Pathophysiologic Approach, 7th ed. New York: McGraw-Hill, 2008.
Gold Standard, Inc. Acamprosate (Indications/Dosage). https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=2097&sec=monindi&t=0. Accessed May 24, 2016.
Reference:
Doering P, Boothby L. Substance-related disorders: overview and depressants, stimulants, and hallucinogens. In: DiPiro J, Talbert R, Yee G, et al., eds. Pharmacotherapy. A Pathophysiologic Approach, 7th ed. New York: McGraw-Hill, 2008.
Gold Standard, Inc. Acamprosate (Indications/Dosage). https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=2097&sec=monindi&t=0. Accessed May 24, 2016.
Question 26 |
Which of the following is/are major risk factors for VTE?
Surgery | |
Cancer | |
A and B | |
Alcohol consumption |
Question 26 Explanation:
Surgery, trauma (major trauma or lower-extremity injury), immobility, lower-extremity paresis, cancer (active or occult), cancer therapy (hormonal, chemotherapy, angiogenesis inhibitors, radiotherapy), venous compression (tumor, hematoma, arterial abnormality), previous VTE, increasing age, pregnancy and the postpartum period, estrogen-containing oral contraceptives or hormone replacement therapy, selective estrogen receptor modulators, erythropoiesis-stimulating agents, acute medical illness, inflammatory bowel disease, nephrotic syndrome, myeloproliferative disorders, paroxysmal nocturnal hemoglobinuria, obesity, central venous catheterization, and inherited or acquired thrombophilia.
Reference:
Prevention of Venous Thromboembolism*: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6_suppl):381S.
Reference:
Prevention of Venous Thromboembolism*: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6_suppl):381S.
Question 27 |
What is/are the indication for Stress Ulcer Prophylaxis (SUP)?
Patients with coagulopathy not related to anticoagulation use | |
Requirement for mechanical Ventilator for over 48hrs | |
Use of high-dose corticosteroids (>250 mg of hydrocortisone or the equivalent per day) | |
All of the above |
Question 27 Explanation:
SUP is indicated for patients who have coagulopathy, a requirement for mechanical ventilation for over 48 hours, a history of GI ulceration or bleeding within one year before admission, and in patients with at least two of the following: ICU stay of more than one week, sepsis, use of high-dose corticosteroids (>250 mg of hydrocortisone or the equivalent per day) and occult bleeding lasting six days or more.
Reference:
ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998. Am J Health Syst Pharm. 1999;56(4):347-379.
Reference:
ASHP Therapeutic Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998. Am J Health Syst Pharm. 1999;56(4):347-379.
Question 28 |
In a study where Rivaroxaban was compared to enoxaparin to find total VTE following HIP replacement surgery, there were 17 total VTE out of 1513 patients in the Rivaraoaban group and 57 total VTE out of 1473 patient in the enoxaparin group. How many patients would you need to treat with rivaroxaban rather than enoxaparin to prevent 1 VTE event?
27 | |
63 | |
36 | |
72 |
Question 28 Explanation:
Number needed to treat: 36
1/(absolute risk reduction) =
1/0.02746 = 36.4166 = 36
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
1/(absolute risk reduction) =
1/0.02746 = 36.4166 = 36
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 29 |
JM is a 66 YOM comes to your clinic complaining of excessive thirst and urination for the past 1 month. His past medical history includes hypertension and dyspepsia. Home medications includes Amlodipine 5mg by mouth daily and Famotidine 20 mg by mouth twice. He is 5 feet 8 inches and weighs 180 pounds. Point of care plasma glucose test was 224 mg/dl. His 2 average blood pressures is 124/78. Which of the following statement is true about JM’s diagnosis of type 2 diabetes(D2M)?
A1C must be above 6.5 % to diagnose him of D2M
| |
2 hours plasma glucose of ≥ 200mg/dl after a 75 gm oral glucose load must be done to diagnose him of D2M | |
Fasting plasma glucose of ≥ 126 mg/dl must be obtained for a diagnosis of D2M | |
JM already has a diagnosis of D2M based on his random plasma glucose of ≥ 200mg/dl and the presence of diabetes mellitus symptoms |
Question 29 Explanation:
This patient’s symptoms of excessive thirst and urination over the past month plus random plasma glucose ≥ 200mg/dl gives him diagnosis for diabetes. Answer choices A, B, and C are also correct options for criteria to meet diagnosis for any patient, however they do not fit this patient specifically. Only one of these 4 criteria has to be met to meet diagnosis. The AACE/ACE 2015 guidelines defines possible symptoms of diabetes mellitus as frequent thirst (polydipsia), frequent urination (polyuria), polyphagia (extreme hunger), blurred vision, weakness, and unexplained weight loss.
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1)
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1)
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113
Question 30 |
Which of the following statements is true regarding piperacillin-tazobactam and ampicillin-sulbactam?
Piperacillin-tazobactam covers Acinetobacter, ampicillin-sulbactam does not. | |
Piperacillin-tazobactam covers ESBL, ampicillin-sulbactam does not. | |
Piperacillin-tazobactam covers pseudomonas, Ampicillin-sulbactam covers Acinetobacter. | |
Neither Piperacillin-tazobactam or ampicillin-sulbactam has anaerobic coverage |
Question 30 Explanation:
A is wrong because ampicillin-sulbactam covers Acinetobacter and piperacillin-tazobactam has variable coverage for Acinetobacter. B. is wrong because neither ampicillin-sulbactam nor piperacillin-tazobactam covers ESBL. D. is wrong because both ampicillin-sulbactam and piperacillin-tazobactam cover anaerobes.
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014.
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014.
Question 31 |
A patient comes in with urosepsis with risk factors for ESBL. What is the best option to start empiric therapy?
Ertapenem | |
Piperacillin-tazobactam | |
Ceftriaxone | |
Ampicillin-sulbactam |
Question 31 Explanation:
Ertapenem is the drug of choice for ESBL empirically due to higher percentage of sensitivity. It can be de-escalated once culture and sensitivity available.
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Question 32 |
A Patient is receiving Piperacillin-Tazobactam for complicated UTI. Her allergies are sulfa and Moxifloxacin.What would be the most appropriate agent for de-escalation based on the C+S report?
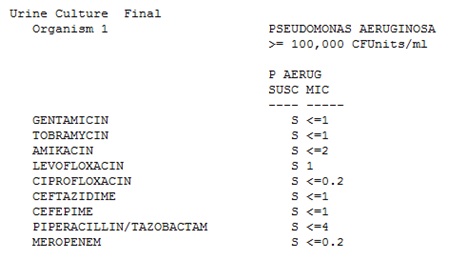
Cefepime | |
Continue piperacillin-tazobactam | |
Ciprofloxacin | |
Meropenem |
Question 32 Explanation:
Cefepime coverage is narrower than that of piperacillin-tazobactam and the culture is sensitive to Cefepime. Ciprofloxacin is not appropriate due to patient’s allergy to moxifloxacin.
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Question 33 |
Which of the following are risk factors for clostridium Difficile?
Advanced age | |
Previous antimicrobial usage | |
Use of acid-suppressing medications. | |
All of the Above |
Question 33 Explanation:
Advanced age, previous antimicrobial usage, duration of hospitalization, cancer chemotherapy, GI surgery, tube feeding, and use of acid-suppressing medications.
Reference:
Cohen S, Gerding D, Johnson S et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431-455. Doi: 10.1086/651706
Reference:
Cohen S, Gerding D, Johnson S et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults: 2010 Update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431-455. Doi: 10.1086/651706
Question 34 |
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure.
Given the data above what is the absolute risk of cardiovascular death with Dronedarone group in severe heart failure patients?0.033 | |
0.077 | |
0.13 | |
0.77 |
Question 34 Explanation:
Absolute risk: 0.077
(Cardiovascular death with Dronedarone)/(Total in Dronedarone group) = 24/310 = 0.077419
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
(Cardiovascular death with Dronedarone)/(Total in Dronedarone group) = 24/310 = 0.077419
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 35 |
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure.
What is the relative risk of cardiovascular death using Dronedarone therapy compared to placebo?2.7 | |
1.7 | |
97.3 | |
98.3 |
Question 35 Explanation:
Relative risk: 2.7
(Event rate in Dronedarone group)/(Event rate in Placebo group) = (24/310)/(9/317) = 2.72688
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
(Event rate in Dronedarone group)/(Event rate in Placebo group) = (24/310)/(9/317) = 2.72688
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 36 |
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure
What is the absolute risk of cardiovascular death in placebo group in severe heart failure patients?0.077 | |
0.082 | |
0.028 | |
0.033 |
Question 36 Explanation:
Absolute risk: 0.028
(Cardiovascular death with Placebo)/(Total in Placebo group) = 9/317 = 0.02839
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
(Cardiovascular death with Placebo)/(Total in Placebo group) = 9/317 = 0.02839
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 37 |
Study that looked at mortality after Dronedarone Therapy for Severe Heart Failure
What is the relative risk increase using Dronedarone compared to placebo in severe heart failure patients?170% | |
30% | |
6.9% | |
4.9% |
Question 37 Explanation:
Relative risk increase: 1.7 = 170%
1 – (relative risk) =
1 – 2.72688 = - 1.72688
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
1 – (relative risk) =
1 – 2.72688 = - 1.72688
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 38 |
According to the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults, which of the following LDL cholesterol thresholds is an indication for high-intensity statin therapy?
≥ 100 mg/dL | |
≥ 130 mg/dl | |
≥ 190 mg/dL | |
≥ 200 mg/dL |
Question 38 Explanation:
Statin therapy should be used as treatment in adults with with primary LDL–C ≥190 mg/dL and age over 21 years. Unless contraindicated, high-intensity statin therapy should be used.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Question 39 |
According to the 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults, which of the following medications and dosing regimens is considered moderate-intensity statin therapy?
Atorvastatin 80 mg PO QHS | |
Lovastatin 20 mg PO QHS | |
Simvastatin 40 mg PO QHS | |
Rosuvastatin 40 mg PO QHS |
Question 39 Explanation:
Moderate-Intensity Statin Therapy:
Atorvastatin 10 (20) mg, Rosuvastatin (5) 10 mg, Simvastatin 20–40 mg, Pravastatin 40 (80) mg, Lovastatin 40 mg, Fluvastatin XL 80 mg, Fluvastatin 40 mg bid, Pitavastatin 2–4 mg
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Atorvastatin 10 (20) mg, Rosuvastatin (5) 10 mg, Simvastatin 20–40 mg, Pravastatin 40 (80) mg, Lovastatin 40 mg, Fluvastatin XL 80 mg, Fluvastatin 40 mg bid, Pitavastatin 2–4 mg
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Question 40 |
Which of the following clinical laboratory tests should be ordered and evaluated if a patient complains of unexplained severe muscle symptoms or fatigue while on statin therapy?
Total Bilirubin | |
Creatine Phosphokinase | |
Complete Blood Count | |
Liver function tests |
Question 40 Explanation:
Creatine Phosphokinase (CPK) should be evaluated if a patient experiences unexplained severe muscle symptoms or fatigue while receiving statin therapy.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Question 41 |
Results from a case-control study where they assessed whether a drug is associated with decrease in weight showed odds ratio for weight change 0.7 (95% CI, 0.6-1.2). How can this data best be interpreted?
The drug increase weight by 30%
| |
The drug decrease weight by 30%
| |
The drug decrease weight by 70%
| |
The data inconclusive to whether the drug is associated with change in weight
|
Question 41 Explanation:
When the 95% CI spans 1 (the null) the results may not be significant. These results would suggest a look into the p-value to determine the significance of these results.
Reference:
Szumilas, M. "Explaining odds ratios." J Can Acad Child Adolesc Psychiatry 19 (2010): 227. Retrieved Jan. 24, 2017 from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2938757
Reference:
Szumilas, M. "Explaining odds ratios." J Can Acad Child Adolesc Psychiatry 19 (2010): 227. Retrieved Jan. 24, 2017 from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2938757
Question 42 |
Which of the following medication may increase LDL?
Lisinopril | |
Hydrochlorothiazide | |
Diltiazem | |
Acetaminophen |
Question 42 Explanation:
LDL can be elevated by diuretics, cyclosporine, glucocorticoids, and amiodarone.
Reference:
I. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013; 129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Reference:
I. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013; 129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a.
Question 43 |
In the ARISTOTLE Study the rate of death from any cause was 3.52% in Apixaban group per year Vs 3.94% in warfarin group. HR 0.89; 95% CI, 0.80 to 0.99. Which of the following statement is true based on the given information?
The rate of death from any cause was lower in the Apixaban group than in Warfarin group. | |
The rate of death from any cause was not significant in the Apixaban group Vs Warfarin group. | |
Warfarin had significantly lower rate of death compared to Apixaban. | |
Since there is no p value no conclusion can be drawn from the given data |
Question 43 Explanation:
A Is correct because the rate of death is significant as indicated by the 95% CI does not contain the value 1. So it is appropriate to make a statement: The rate of death from any cause was lower in the Apixaban group than in Warfarin group the meaning of 1 in a confidence ration indicates that the risk reduction in the outcome is the same between the two groups. Answer C is wrong because the rate of death in the warfarin group was higher than the rate in the Apixaban group (3.94% vs 3.52% perspectively). Answer D is wrong because although there is no p value listed, statistical significance can still be inferred from a 95% confidence interval, which is presented here as 0.80 to 0.99.
Reference:
Windish DM, Huot SJ, Green ML. Medicine resident’s understanding of the biostatistics and results in the medical literature. JAMA 2007;298:1010-22.
Reference:
Windish DM, Huot SJ, Green ML. Medicine resident’s understanding of the biostatistics and results in the medical literature. JAMA 2007;298:1010-22.
Question 44 |
In the ARISTOTLE Study the rate of the primary outcome was 1.27% per year in the Apixaban group, as compared with 1.60% per year in the Warfarin group (hazard ratio with Apixaban, 0.79; 95% confidence interval [CI], 0.66 to 0.95; P<0.001 for noninferiority. The primary objective was to determine whether Apixaban was noninferior to Warfarin in reducing the rate of stroke (ischemic or hemorrhagic) or systemic embolism among patients with atrial fibrillation and at least one other risk factor for stroke. Which of the following statement is true based on the given information?
Apixaban is superior to warfarin in reducing rate of stroke or systemic embolism among patients with atrial fibrillation. | |
Apixaban is as effective as warfarin in reducing rate of stroke or systemic embolism among patients with atrial fibrillation. | |
Apixaban is more effective than warfarin in reducing rate of stroke but not systemic embolism among patients with atrial fibrillation | |
Apixaban is superior to warfarin in reducing rate of stroke but warfarin is noninferior in reducing systemic embolism among patients with atrial fibrillation. |
Question 44 Explanation:
Answer A is incorrect because presented p-value is for noninferiority, not for superiority. Based on the given information, no conclusions about superiority can be made. Answer B. is correct. The p-value provided is for noninferiority, it can be concluded that Apixaban is as effective as warfarin in reducing rate of stroke or systemic embolism among patients with atrial fibrillation. Answer C is incorrect. Stroke and systemic embolism were combined into one primary outcome here for this confidence interval, so more information is needed to determine which agent did better for the specific type of event, either stroke or systemic embolism. Answer D. is incorrect because the rate of the primary outcome was higher in the warfarin group compared to the Apixaban group, meaning stroke or systemic embolism occurred more so in the warfarin group. For the same reason as with C, these two events are represented as combined into one primary outcome and more information would be needed.
Reference: I. Windish DM, Huot SJ, Green ML. Medicine resident’s understanding of the biostatistics and results in the medical literature. JAMA 2007;298:1010-22.
Reference: I. Windish DM, Huot SJ, Green ML. Medicine resident’s understanding of the biostatistics and results in the medical literature. JAMA 2007;298:1010-22.
Question 45 |
PW is a 46 year African American man with a history of Chronic Kidney Disease due to radiocontrast media. His two average BP readings are 157/94 mm Hg, HR is 65 beats per minute. His CBC and CMP are within normal limits, except serum creatinine is 1.6mg/dL. Which of the following is the best way to manage her hypertension according to the Eight Joint National Committee (JNC 8)?
Lifestyle modification | |
Lifestyle modification and lisinopril 2.5mg daily | |
Lifestyle modification and amlodipine 2.5mg daily | |
Life style modification and metoprolol succinate 25md daily |
Question 45 Explanation:
The patient is less than 60 years old, African American, and has CKD. Therefore, his goal BP should be SBP < 140 mmHg and DBP < 90 mmHg. In the population aged ≥18 years with CKD, initial (or add-on) antihypertensive treatment should include an ACEI or ARB to improve kidney outcomes. This applies to all CKD patients with hypertension regardless of race or diabetes status. (Moderate Recommendation – Grade B) His heart rate is on the lower end of the normal range of 60-80, so adding metoprolol succinate would not be an ideal option.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Question 46 |
A 65 years old Caucasian man with a history of hypertension, hypercholesterolemia presents to your clinic. Despite of him being compliant on medication and lifestyle changes his two average BP readings are 167/107 mm Hg, HR is 88. His current medication includes Valsartan 320mg daily, atorvastatin 80mg daily, hydrochlorothiazide 25mg daily and Amlodipine 10mg daily. His CBC and CMP are within normal limits. Which of the following is the best medication to add?
Metoprolol succinate 25mg oral daily | |
Chlorthalidone 25mg oral daily | |
Lisinopril 40mg oral daily | |
Nifedipine 30mg Extended release oral daily |
Question 46 Explanation:
This patient is over the age of 60, and he does not have any diabetes or CKD, so his goal BP should be SBP < 150 mmHg, and DBP< 90 mmHg. He is currently taking an ARB (Valsartan), so he should not receive lisinopril since the combined use of an ACE inhibitor and an ARB should be avoided. This patient is currently taking three hypertension drugs. Since a fourth drug is needed, drugs from classes other than thiazide-type diuretics, CCBs ACEIs, or ARBs can be used. The option that fits this is A, metoprolol succinate, because it is a beta blocker.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Question 47 |
A 37 years old Caucasian Man with no past medical history presents to your clinic. His two average BP readings are 146/87 mm Hg, HR is 65. His CBC and CMP are within normal limits. Which of the following is the best way to manage her hypertension according to the Eight Joint National Committee (JNC 8)?
Lifestyle modification only | |
Lifestyle modification and amlodipine 2.5mg daily | |
Life style modification and hydrochlorothiazide 25mg daily | |
B or C, both are appropriate |
Question 47 Explanation:
The patient is under the age of 60 and is considered a member of the general population since there is no known history, and he is Caucasian. JNC8 does not address definitions of hypertension and prehypertension, but defines the threshold for initiating pharmacologic therapy. Medications should be started when SBP is 140 mmHg or higher. For Caucasian patients, either a thiazide-type diuretic, an ACEI or ARB, or a CCB should be initiated. Both choices B and C are appropriate options at appropriate starting doses.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427.
Question 48 |
In a study where Rivaroxaban was compared to Enoxaparin to find total VTE following HIP replacement surgery, there were 17 total VTE out of 1513 patients in the Rivaraoaban group and 57 total VTE out of 1473 patient in the enoxaparin group. What is the relative risk reduction of using Rivaroxaban over Enoxaparin?
17 | |
57 | |
71 | |
2.7 |
Question 48 Explanation:
Relative risk reduction: 0.71 = 71%
Relative risk: (Event rate in Rivaroxaban group)/(Event rate in Enoxaparin group) = (17/1513)/(57/1473) = 0.2903 Relative risk reduction: 1 – (relative risk) = 1 – 0.2903 = 0.7097 = 0.71
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Relative risk: (Event rate in Rivaroxaban group)/(Event rate in Enoxaparin group) = (17/1513)/(57/1473) = 0.2903 Relative risk reduction: 1 – (relative risk) = 1 – 0.2903 = 0.7097 = 0.71
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 49 |
In a study where Rivaroxaban was compared to Enoxaparin to find total VTE following HIP replacement surgery, there were 17 total VTE out of 1513 patients in the Rivaraoaban group and 57 total VTE out of 1473 patient in the enoxaparin group. What is the absolute risk reduction of using Rivaroxaban over Enoxaparin?
17 | |
57 | |
71 | |
2.7 |
Question 49 Explanation:
Absolute risk reduction: 0.027 = 2.7%
(Event rate in enoxaparin group) – (Event rate in rivaroxaban group) = (57/1473) – (17/1513) = 0.02746
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
(Event rate in enoxaparin group) – (Event rate in rivaroxaban group) = (57/1473) – (17/1513) = 0.02746
Reference:
Barratt A, Wyer PC, Hatala R, et al. Tips for learners of evidence-based medicine: 1. Relative risk reduction, absolute risk reduction and number needed to treat. CMAJ. 2004;171(4):353-8. doi: 10.1503/cmaj.1021197.
Question 50 |
Which of the following is/are Categorical data?
Age | |
Sex | |
Better/Same /Worse | |
B and C. |
Question 50 Explanation:
Categorical data includes ordinal (ordered categories) and nominal (unordered categories). Age is not categorical because age can fall under any continuous number, so it is considered quantitative, continuous data. Sex is nominal categorical data. Better/same/worse is considered ordinal categorical since the answers fall in order.
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 51 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
Which of the following is the best initial approach for his management of acute pancreatiits?
Early aggressive intravenous hydration with Lactate Ringer.
| |
Early aggressive intravenous hydration with Normal Saline.
| |
Early aggressive intravenous hydration with Dextrose 5%.
| |
Early aggressive oral hydration with electrolyte balanced drink.
|
Question 51 Explanation:
Aggressive hydration defined, as 250-500mL/hr of isotonic crystalloid solution should be provided to all patients, unless cardiovascular and/or renal comorbidities exist. Lactated Ringer’s solution may be the preferred isotonic crystalloid replacement fluid. Lactated Ringer’s solution appears to be more beneficial, resulting in fewer patients developing SIRS as compared with patients receiving normal (0.9%) saline. Thus, D and B, and C are incorrect.
Reference:
Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013
Reference:
Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013
Question 52 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
Which of the following is/ are true statement regarding antibiotics use in acute pancreatitis?
Antibiotics should be given for an extrapancreatic infection. | |
Prophylactic antibiotics should be given to all patients with acute pancreatitis. | |
Antibiotic should be given to patients with sterile necrosis.
| |
All are true.
|
Question 52 Explanation:
Antibiotics should be given for an extrapancreatic infection, such as cholangitis, catheter-acquired infection, bacteremia, urinary tract infection, and pneumonia. Routine use of prophylactic antibiotics in patients with severe acute pancreatitis is not recommended. The use of antibiotics in patients with sterile necrosis to prevent the development of infected necrosis is not recommended. Also, routine use of prophylactic antibiotics in patients with severe acute pancreatitis is not recommended. Thus, B, C, and D are incorrect.
Reference:
Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013
Reference:
Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013
Question 53 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
Which of the following drug ME is on, have reported cases of pancreatitis?
Excenatide | |
Ranitidine
| |
Cholestyramine
| |
All of the above |
Question 53 Explanation:
All of the above medications has reported cases of pancreatitis.
Reference:
I. Kaurich T., Drug-Induced acute pancreatitis, Proc (Bayl Univ Med Cent). 2008 Jan; 21(1): 77–81. Availbale at: www.ncbi.nlm.nih.gov/pmc/articles/PMC2190558/. Accessed September 29, 2016.
II. Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013. Availbale at: https://gi.org/guideline/acute-pancreatitis/ . Accessed September 29, 2016.
Reference:
I. Kaurich T., Drug-Induced acute pancreatitis, Proc (Bayl Univ Med Cent). 2008 Jan; 21(1): 77–81. Availbale at: www.ncbi.nlm.nih.gov/pmc/articles/PMC2190558/. Accessed September 29, 2016.
II. Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013. Availbale at: https://gi.org/guideline/acute-pancreatitis/ . Accessed September 29, 2016.
Question 54 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
Which of the following is most likely cause of ME’s acute pancreatitis?
Blood Glucose of 380mg/dl
| |
Triglyceride of 1751 mg/dl
| |
Lipase 2976 units/L
| |
Calcium of 6.0mg/dl |
Question 54 Explanation:
In the absence of gallstones and/or history of significant alcohol use, a serum triglyceride should be obtained and considered the etiology if >1,000 mg/dL or high calcium level in the blood.Patient’s triglyceride level is 1751 mg/dL, Primary and secondary hypertriglyceridemia can cause
acute pancreatitis. Serum lipase has a sensitivity and specificity for acute pancreatitis and may rise within 4-8 hours of the onset of symptoms, and peak at 24 hours.Thus answers A, B, and D are
incorrect.
Reference: Acute Pancreatitis. UpToDate. 2016. Available at: https://www.uptodate.com/contents/etiology-of-acute-pancreatitis . Accessed September 29, 2016
Reference: Acute Pancreatitis. UpToDate. 2016. Available at: https://www.uptodate.com/contents/etiology-of-acute-pancreatitis . Accessed September 29, 2016
Question 55 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
What is the first-line agent for prevention of Hypertriglyceridemia-induced acute pancreatitis?
Niacin
| |
Fibrates
| |
Insulin
| |
Statin |
Question 55 Explanation:
Patients with very high triglyceride levels (i.e., 500mg/dL or higher) usually require drug therapy in addition to therapeutic lifestyle changes. Fibrates or niacin is practical first0line choices for these patients. The initial goal is to decrease the risk of acute pancreatitis, especially if triglyceride levels are above 1,000mg/dL. Fibrate therapy can reduce triglyceride level by 20-50%, whereas nicotinic acid can reduce triglycerides at a much lower dose ~ 15-25%. Thus, A is incorrect. For patients with a triglyceride level below 500 mg/dL (5.7 mmol/L) in whom pharmacologic therapy is indicated, we suggest treatment with a statin rather than an agent targeted at reduction of triglycerides. Thus, D is incorrect. Insulin therapy is initiated for acute pancreatitis treatment, thus C is incorrect.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Question 56 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
When Apheresis is unavailable, besides aggressive hydration, what is optimal alternative for treatment of Hypertriglyceridemia-induced acute pancreatitis?
Continuous intravenous insulin infusion with blood sugar parameters.
| |
Heparin 5000 units subcutaneous twice daily
| |
Short duration of high dose of fenofibrates
| |
Short duration of high dose of statin |
Question 56 Explanation:
Answers C and D are incorrect, as they are utilized for preventative care. If apheresis is unavailable, or if the patient cannot tolerate apheresis, or if the patient's serum glucose level is >500 mg/dL, a continuous IV insulin infusion is initiated. Typically IV infusion of regular insulin is started at a rate of 0.1 to 0.3 units/kg/hour. In patients with blood sugar levels between 150 and 200 mg/dL, IV glucose supplementation with a separate 5 percent dextrose infusion to prevent hypoglycemia due to the insulin infusion is started. The serum glucose should initially be measured every hour to monitor glucose levels and the insulin infusion should be adjusted accordingly. Triglyceride levels should be monitored every 12 to 24 hours with adjustment of the insulin dosage as needed. Intravenous insulin should be stopped when triglyceride levels are <500 mg/dL, which typically occurs within a few days. Heparin’s use is controversial and is not recommended, thus B is incorrect.
Reference:
I. Hypertriglyceridemia-induced Acute Pancreatitis. UpToDate. 2016. Available at: https://www.uptodate.com/contents/ hypertriglyceridemia-induced-acute-pancreatitis Accessed September 29, 2016. II. Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013. Available at: https://gi.org/guideline/acute-pancreatitis/ Accessed September 29, 2016.
Reference:
I. Hypertriglyceridemia-induced Acute Pancreatitis. UpToDate. 2016. Available at: https://www.uptodate.com/contents/ hypertriglyceridemia-induced-acute-pancreatitis Accessed September 29, 2016. II. Management of Acute Pancreatitis, Am J Gastroenterol 2013; 108:1400–1415; doi:10.1038/ajg.2013.218; published online 30 July 2013. Available at: https://gi.org/guideline/acute-pancreatitis/ Accessed September 29, 2016.
Question 57 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
Physician orders to give magnesium sulfate 2gm intravenously, potassium chloride 40meq intravenously, sodium phosphate 15 mmol intravenously and Calcium chloride 2gm intravenously. Which of the following electrolytes should not be infused together in the same intravenous line?
Magnesium sulfate 2gm intravenously and Potassium chloride 40meq intravenously.
| |
Sodium phosphate 15 mmol intravenously and Calcium chloride 2gm intravenously.
| |
Potassium chloride 40meq and Calcium chloride 2gm intravenously
| |
Magnesium sulfate 2gm intravenously and Calcium chloride 2gm intravenously. |
Question 57 Explanation:
Answer B. Calcium salts and phosphates are inherently incompatible and will precipitate, thus one should not infusing sodium phosphate and calcium chloride together in the same intravenous line.
Reference:
Clinical Pharmacology. Retrieved December 10, 2016, from http://www.clinicalpharmacology-ip.com/Forms/Reports/ivreport.aspx
Reference:
Clinical Pharmacology. Retrieved December 10, 2016, from http://www.clinicalpharmacology-ip.com/Forms/Reports/ivreport.aspx
Question 58 |
ME is a 65 YOM with past medical history of HTN, DM, hyperlipidemia and BPH, comes through the ER with sever bilateral upper quadrant and epigastric abdominal pain associated with nausea. NKDA and weighs 80 Kg. CT abdomen and pelvis with contrast confirmed advanced pancreatitis. His home medication includes Tamsulosin, Metformin, Exenatide, Ranitidine, Cholestyramine and Losartan. Pertinent labs incudes Lipase 2976 units/L, HDL 29mg/dl, LDL 79 mg/dl, Cholesterol 355mg/dl, triglyceride 1751mg/dl, calcium 6.0mg/dl, Albumin 2.3g/dl, Magnesium 1.4mg/dl, Potassium 3.6. Sodium 131 mmol/L, Phosphorus 2.0mg/dl Serum Creatinine 1.1 mg/dl, BG 380 mg/dl and WBC 7.9 x1000/ul. Vitals: RR 16, Pulse 117, Temperature 100.5 F, Blood Pressure 138/73 mm Hg, pulse oximetry 98%.
What is ME’s corrected calcium?
7.36
| |
8.3
| |
10
| |
9.1 |
Question 58 Explanation:
Corrected Calcium Formula: Serum calcium + 0.8 (4- serum Albumin)
6.0 + 0.8 (4-2.3) = 7.36
Reference:
EBM Consult : Calcium Correction for Hypoalbuminemia Medical Calculator. Ebmconsultcom. 2016. Available at: http://www.ebmconsult.com/app/medical-calculators/calcium-correction-albumin-calculator Accessed September 30, 2016.
6.0 + 0.8 (4-2.3) = 7.36
Reference:
EBM Consult : Calcium Correction for Hypoalbuminemia Medical Calculator. Ebmconsultcom. 2016. Available at: http://www.ebmconsult.com/app/medical-calculators/calcium-correction-albumin-calculator Accessed September 30, 2016.
Question 59 |
Which of the following if true regarding intravenous calcium gluconate 1gm and intravenous calcium chloride 1gm?
Calcium gluconate provides 4.65 mEq per gram of elemental calcium and calcium chloride provides 13.6 mEq per gram of elemental calcium.
| |
Calcium gluconate 1gm and calcium chloride 1gm both provide 4.65 mEq per gram of elemental calcium.
| |
Calcium gluconate provides 13.6 mEq per gram of elemental calcium and calcium chloride provides 4.65 mEq per gram of elemental calcium.
| |
Calcium gluconate 1gm and calcium chloride 1gm both provide 13.6 mEq per gram of elemental calcium. |
Question 59 Explanation:
1g of calcium chloride (10mL) = 13.6mEq of elemental calcium
1g of calcium gluconate (10mL) = 4.65mEq of elemental calcium
Reference:
CALCIUM CHLORIDE - Intravenous (IV) Dilution. Globalrphcom. 2016. Available at: http://www.globalrph.com/calcium_dilution.htm . Accessed September 30, 2016.
1g of calcium gluconate (10mL) = 4.65mEq of elemental calcium
Reference:
CALCIUM CHLORIDE - Intravenous (IV) Dilution. Globalrphcom. 2016. Available at: http://www.globalrph.com/calcium_dilution.htm . Accessed September 30, 2016.
Question 60 |
There were total of 510 cases of syphilis with 106 reported new case of syphilis in Dresner County in 2015. The population of Dresner County in 2015 was 410,200 people.
What is the incidence proportion of syphilis in 2015 in Dresner County?
0.026%
| |
0.153%
| |
0.051%
| |
0.015% |
Question 60 Explanation:
Incidence proportion = New reported cases / initial population at risk
Incidence proportion = 106 / (410,200 – 510) = 0.000259 x 100 = 0.026%
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
Incidence proportion = 106 / (410,200 – 510) = 0.000259 x 100 = 0.026%
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
Question 61 |
There were total of 510 cases of syphilis with 106 reported new case of syphilis in Dresner County in 2015. The population of Dresner County is 410,200 people.
What is the incidence rate of syphilis in 2015 in Dresner County?
2.6 cases per 10,000 person-years
| |
2.3 cases per 10,000 person-years
| |
2 cases per 10,000 person-years
| |
3.2 cases per 10,000 person-years |
Question 61 Explanation:
Incidence rate = New reported cases / summed person-years of observation (avg population during time interval)
410,200 – 510 = 409,690 – 106 = 409,584
Incidence rate = 106 / (409,584 + ½ 106) = 2.6 cases per 10,000 person-years
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
410,200 – 510 = 409,690 – 106 = 409,584
Incidence rate = 106 / (409,584 + ½ 106) = 2.6 cases per 10,000 person-years
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
Question 62 |
Which of the following beta-blocker is NOT proven to reduce mortality in patients with Systolic CHF?
Bisoprolol
| |
Nadolol
| |
Carvedilol
| |
Metoprolol succinate |
Question 62 Explanation:
Nadolol is not proven to reduce mortality in patients with systolic CHF. The efficacy of nadolol in HF has not been determined. For patients taking nadolol, it should be used with caution in those with compensated heart failure and patients should be monitored for a worsening of the condition.
Bisoprolol, carvedilol, and sustained-release metoprolol succinate are the beta-blockers that have been proven to reduce mortality in patients with systolic CHF. These 3 beta-blockers have been effective in reducing the risk of death in patients with chronic HFrEF. Other beta-blockers were found to be less effective. Bucindolol did not exhibit uniform effectiveness across different populations. Metoprolol tartrate was found to be less effective in HF clinical trials.
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Question 63 |
TM is a 78 YOW with a history of hypertension, hypercholesterolemia and arthritis was admitted for proximal arterial fibrillation. While in the hospital she was placed on diltiazem drip and eventually, converted to oral diltiazem 240mg. Pt’s home medication includes Simvastatin 40mg po daily , hydrochlorothiazide 25mg po daily , Lisinopril 20mg daily and Acetaminophen. Her LDL-C is 100mg /dL. What would be the most appropriate change to make on her therapy?
Increase Simvastatin to 80mg po daily
| |
Keep Simvastatin at 40mg po daily
| |
Change Simvastatin 40mg to Atorvastatin 40mg po daily
| |
Change Simvastatin to Lovastatin 20mg po daily |
Question 63 Explanation:
Answer C. Diltiazem has a major drug interaction with Simvastatin. Diltiazem is a CYP3A4 inhibitor, and since Simvastatin is metabolized by CYP3A4, its level can build up and the risk of myopathy increases. It is recommended to switch to a non-CYP3A inhibitor such as Pitavastatin, Pravastatin, or Rosuvastatin, and if Simvastatin is to be kept on it should not exceed 10 mg/day. The same interaction also exists with lovastatin, and the recommendation is to not exceed a total dose of 20 mg/day po of Lovastatin. Given the current options, the best choice is to change to Atorvstatin 40 mg po daily.
Reference:
I. FDA Drug Safety Communication: New restrictions, contraindications, and dose limitations for Zocor (simvastatin) to reduce the risk of muscle injury. December 15, 2011. Retrieved on Feb 8th, 2017 from : http://www.fda.gov/Drugs/DrugSafety/ucm256581.htm
II. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Reference:
I. FDA Drug Safety Communication: New restrictions, contraindications, and dose limitations for Zocor (simvastatin) to reduce the risk of muscle injury. December 15, 2011. Retrieved on Feb 8th, 2017 from : http://www.fda.gov/Drugs/DrugSafety/ucm256581.htm
II. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Question 64 |
What is the optimal duration of antibiotic therapy for HAP and VAP?
5 days
| |
7 days
| |
10 days
| |
14 days |
Question 64 Explanation:
Answer B. Short-course antibiotic therapy is associated with less antibiotic exposure and antibiotic resistance. This would result in reduced costs and side effects. The benefits of therapy are not reduced with a shorter duration.
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Question 65 |
PM is a 62 YOM who has never received zoster vaccine. When he was 57 year old he had an episode of herpes zoster. He wants to know if he is a candidate for zoster vaccine. Which of the following statement is true?
No he is not a candidate for zoster vaccine since he already had herpes zoster and has built immunity to it.
| |
Yes he is still candidate for zoster vaccine regardless of his prior episode of herpes zoster.
| |
No he is not a candidate, since it is recommended for patients who are 65 years old and above.
| |
No he is not a candidate since it is only indicated for patients who are under 60 years of age. |
Question 65 Explanation:
A single dose of zoster vaccine is recommended for all adults 60 years or older, regardless of whether they report a prior episode of herpes zoster, thus A is wrong. Also, although 2nd and 3rd episodes of herpes zoster can occur, the annual incidence of recurrence is not known. Although the FDA recommends the administration of the vaccine for individuals 50 years or older, the ACIP recommends that vaccinations begin at 60 years, thus C and D are incorrect.
Reference:
I. Shingles | Clinical Overview - Varicella Vaccine | Herpes Zoster | CDC. Cdcgov. 2016. Available at: http://www.cdc.gov/shingles/hcp/clinical-overview.html. Accessed September 27, 2016.
II. Adult Immunization Schedule. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated April 20, 2016. Accessed September 27, 2016
Reference:
I. Shingles | Clinical Overview - Varicella Vaccine | Herpes Zoster | CDC. Cdcgov. 2016. Available at: http://www.cdc.gov/shingles/hcp/clinical-overview.html. Accessed September 27, 2016.
II. Adult Immunization Schedule. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated April 20, 2016. Accessed September 27, 2016
Question 66 |
JP 77 YOW with a history of hypertension, just got admitted for Ischemic Stroke what would be the most appropriate pharmacotherapy recommendation upon discharge?
Atorvastatin 20 mg PO QHS
| |
Pitavastatin 1 mg PO QHS
| |
Atorvastatin 80 mg PO QHS
| |
Lovastatin 20 mg PO QHS |
Question 66 Explanation:
Answer C. A stroke falls under the category of clinical ASCVD, which includes includes acute coronary syndromes, or a history of MI, stable or unstable angina, coronary or other arterial revascularization, stroke, TIA, or peripheral arterial disease presumed to be of atherosclerotic origin. Patients with clinical ASCVD are at an increased risk for recurrent ASCVD and ASCVD death. This patient is under 75 years old, and such patients with clinical ASCVD should receive moderate-intensity statin therapy. However, ATP4 acknowledges that the older patients in the corresponding RCTs were likely to be healthier than those in the general population, so treatment can be individualized. Given the options above, a high intensity statin is the most appropriate option. The decision to start at the 80 mg dose of atorvastatin instead of the 40 mg dose is based on the recommendation to down titrate if the patient is unable to tolerate the 80 mg dose as opposed to up-titrating in accordance with the IDEAL trial.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Question 67 |
Due to contamination of water supply in a small town there were several outbreak of gastroenteritis. 1650 people drank the supply water of which 250 had gastroenteritis, 1540 people drank the bottled water of which 3 people had gastroenteritis. Construct a contingency table. What is the odds ratio(OR)? What is the relative risk(RR)?
OR=17.85, RR=15.15
| |
OR=91.5, RR=77.78
| |
OR=8.7, RR=7.83
| |
OR=0.21, RR=0.19 |
Question 67 Explanation:
No Gastroenteritis Gastroenteritis
Water Supply 1400 250
Bottled Water 1537 3
Risk Ratio = Rate of Gastroenteritis in patients drinking water supply / rate in patients drinking bottled
RR = (250/1650) / (3/1540) = 77.78
Odds = Number of patients with illness / Number of patients without illness
Odds ratio = One group / Other group
Odds ratio = (250/1400) / (3/1537) = 91.5
Another formula used for the odds ratio is: Odds ratio = (exposed cases / unexposed cases) / (exposed non-cases / unexposed non-cases)
In this equation exposed patients are patients that drank from the water supply and unexposed patients are patients that drank from water bottles. Cases are patients that had gastroenteritis and non-cases are patients that did not have the illness present.
Reference:
I. Szumilas, M. "Explaining odds ratios." J Can Acad Child Adolesc Psychiatry 19 (2010): 227. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2938757/ II. 2x2 Contingency Table with Odds Ratios, etc. (n.d.). Retrieved Jan. 24, 2017 from: http://www.vassarstats.net/odds2x2.html
Water Supply 1400 250
Bottled Water 1537 3
Risk Ratio = Rate of Gastroenteritis in patients drinking water supply / rate in patients drinking bottled
RR = (250/1650) / (3/1540) = 77.78
Odds = Number of patients with illness / Number of patients without illness
Odds ratio = One group / Other group
Odds ratio = (250/1400) / (3/1537) = 91.5
Another formula used for the odds ratio is: Odds ratio = (exposed cases / unexposed cases) / (exposed non-cases / unexposed non-cases)
In this equation exposed patients are patients that drank from the water supply and unexposed patients are patients that drank from water bottles. Cases are patients that had gastroenteritis and non-cases are patients that did not have the illness present.
Reference:
I. Szumilas, M. "Explaining odds ratios." J Can Acad Child Adolesc Psychiatry 19 (2010): 227. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2938757/ II. 2x2 Contingency Table with Odds Ratios, etc. (n.d.). Retrieved Jan. 24, 2017 from: http://www.vassarstats.net/odds2x2.html
Question 68 |
DM is a 75 YOW with a history of systolic heart failure who presents to the ER with a 5 days history of progressive worsening of shortness of breath. Her pro-B-Natriuretic Peptide is 28869 pg/ml, Chest X-ray shows: Cardiomegaly with pulmonary vascular congestion and atelectatic changes in the left mid lung. Bilateral pleural effusions. No chills or fevers. Her 2 average BP is 135/92, HR 72. Current medication is enalapril 20mg oral daily, carvedilol 6.5mg orally twice daily.
Which of the following would be the immediate course of action?
Lasix 40mg intravenously twice daily and monitor fluid status | |
Increase enalapril to 40mg oral twice daily | |
Increase Carvediolol to 25mg orally twice daily | |
Give normal saline at 100mls/hr |
Question 68 Explanation:
Initiating Lasix 40 mg IV twice daily would be the immediate course of action in order to improve symptoms of fluid retention. Fluid status would be monitored.Normal saline would not be given. DM would most likely have fluid restricted (1.5 to 2 L per day) to reduce congestive symptoms. For enalapril, the max dose is 20 BID for the treatment of heart failure. Increasing Enalapril would not improve symptoms of heart failure in the short term. Carvedilol would not be increased until after the patient is stable and IV diuretics stopped as well as any vasodilators and inotropic agents.
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Question 69 |
DM is a 75 YOW with a history of systolic heart failure who presents to the ER with a 5 days history of progressive worsening of shortness of breath. Her pro-B-Natriuretic Peptide is 28869 pg/ml, Chest X-ray shows: Cardiomegaly with pulmonary vascular congestion and atelectatic changes in the left mid lung. Bilateral pleural effusions. No chills or fevers. Her 2 average BP is 135/92, HR 72. Current medication is enalapril 20mg oral daily, carvedilol 6.5mg orally twice daily.
4 days later DM is on max dose of furosemide of 120mg iv q12h and metolazone 10mg daily, despite of these diuretics her chest x-ray still show pulmonary edema, her urine output has decreased, now she requires more oxygen, her creatinine clearance has gone up to 3.0. Which of the following medication would be most appropriate to initiate when DM is maxed out on diuretics?
Sodium nitroprussside
| |
Dobutamine
| |
Nitroglycerin
| |
Nesiritide |
Question 69 Explanation:
Nitroglycerin would be the most appropriate to initiate when DM is maxed out on diuretics. IV nitroglycerin helps to rapidly reduce pulmonary congestion. There is also no dosage adjustments provided for renal impairment.
Sodium nitroprusside can also dilate pulmonary vasculature. However, in patients with renal impairment, there is a risk of thiocyanate accumulation and toxicity. Nesiritide has a longer half-life compared to nitroglycerin and nitroprusside and may result in adverse effects occurring for a longer period of time, such as hypotension. Studies have also indicated that patients may be at risk for worsening renal function and increased mortality while taking nesiritide. A recent meta-analysis indicated that there was no significant increase in mortality. When compared to placebo, there was no increased risk of mortality in those treated with nesiritide. However, it is associated with an increased risk of cardiovascular adverse events such as bradycardia and hypotension. Dobutamine would not be used in this case. It would be used as short-term management in those with cardiac decompensation in order to maintain perfusion and preserve end-organ performance in those with cardiogenic shock; bridge therapy in those with stage D heart failure who are unresponsive to guideline-directed medical therapy and device therapy awaiting a heart transplant or mechanical circulatory support; treat those with severe systolic dysfunction who present with low blood pressure and significantly depressed cardiac output, or to provide palliative therapy in select patients. The guidelines also stated that intermittent IV positive inotropic therapy has no proven value in patients with stage C heart failure.
Reference:
I. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
II. Nesiritide. In: Clinical Pharmacology [database on the Internet]. Tampa (FL): Gold Standard; 2016 [updated 2 Aug 2010; cited 2 Sept 2016]. Available from: www.clinicalpharmacology.com
III. Gong B, Wu Z, Li Z. Efficacy and safety of nesiritide in patients with decompensated heart failure: a meta-analysis of randomised trials. BMJ Open. 2016;6(1):e008545. doi: 10.1136/bmjopen-2015-008545.
Reference:
I. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
II. Nesiritide. In: Clinical Pharmacology [database on the Internet]. Tampa (FL): Gold Standard; 2016 [updated 2 Aug 2010; cited 2 Sept 2016]. Available from: www.clinicalpharmacology.com
III. Gong B, Wu Z, Li Z. Efficacy and safety of nesiritide in patients with decompensated heart failure: a meta-analysis of randomised trials. BMJ Open. 2016;6(1):e008545. doi: 10.1136/bmjopen-2015-008545.
Question 70 |
DM is a 75 YOW with a history of systolic heart failure who presents to the ER with a 5 days history of progressive worsening of shortness of breath. Her pro-B-Natriuretic Peptide is 28869 pg/ml, Chest X-ray shows: Cardiomegaly with pulmonary vascular congestion and atelectatic changes in the left mid lung. Bilateral pleural effusions. No chills or fevers. Her 2 average BP is 135/92, HR 72. Current medication is enalapril 20mg oral daily, carvedilol 6.5mg orally twice daily.
An Echocardiogram was ordered Ejection fraction was estimated in the range of 25-30%. DM feels much better her SOB is improved. Her 2 average BP is 142/92, HR 72. All the diuretics have been stopped. Her hemodynamics are stable. What would be the next appropriate course of action?
Increase the Carvedilol to 12.5mg orally twice daily
| |
Increase enalapril to 40mg orally daily
| |
Add digoxin 0.25mg orally daily
| |
Change carvedilol 3.25mg to metoprolol tartare 25mg orally twice daily |
Question 70 Explanation:
The next appropriate course of action would be to increase Carvedilol. Since all diuretics have been stopped and her hemodynamics stable, initiating a beta-blocker is appropriate. The dose would be gradually increased every 2 weeks to the highest dose tolerable. She would also be monitored for congestive signs and symptoms of HF
Digoxin would not be added. Even though digoxin can improve symptoms in mild to moderate HF, long-term treatment had no effect on mortality. It does have the potential to decrease hospitalizations for HF. Carvedilol would not be changed to metoprolol tartrate since metoprolol tartrate was found to be less effective in patients with heart failure. Enalapril would not be increased.
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Reference:
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Question 71 |
Proportion of people in a population who have a particular disease at a specified point in time or over a specified period of time is definition as which of the following?
Incidence rate
| |
Prevalence rate
| |
Mortality rate
| |
Relative risk |
Question 71 Explanation:
Incidence rate = New reported cases / summed person-years of observation (avg population during time interval)
Prevalence = Cases in a population in a given time period / total population at that time
Reference:
I. Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
II. Numerators, denominators and populations at risk. Jun. 20, 2010. Retrieved Jan. 24, 2017 from: http://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/numerators-denominators-populations
Reference:
I. Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
II. Numerators, denominators and populations at risk. Jun. 20, 2010. Retrieved Jan. 24, 2017 from: http://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/numerators-denominators-populations
Question 72 |
PG is a 86 YOW, weight 182 pounds, height 5’10”. Past medical history of hypertension, GI bleed, osteoarthritis, renal failure stage 4 (GFR = 15-30 mL/min), CHF with preserved ejection fraction. Her BP is 142/ 92, A1c 9.3. Her current Metformin 500mg by mouth BID, Insulin glargine 20 units SQ at bedtime, Atorvastatin 20mg by mouth daily, Lisinopril 5mg by mouth daily, Diltiazem 360mg daily, pantoprazole 40mg BID, Acetaminophen 650mg q6hr.
Which of the following would be the most appropriate option for management of his type 2 diabetes Mellitus?
Discontinue Metformin, add Pioglitazone 30mg by mouth daily
| |
Discontinue Metformin, add Empagliflozin 10mg by mouth daily
| |
Discontinue Metformin, add Exenatide 2mg SQ once weekly
| |
Discontinue Metformin and Increase Insulin glargine 30 units and add 5 units Lispro subcutaneously TID |
Question 72 Explanation:
Pioglitazone is not a good option since it can exacerbate his CHF and caries a black box warning. Empagliflozin is not a good option since it is contraindicated in patients with eGFR <30. Exenatide use is not recommended in patients with CrCL<30 mls/hr. Exenatide is not a good option because the patient’s hx of GI bleed is a precaution for use since the drug can slow gastric emptying. Increasing patient’s long acting insulin and adding low dose short acting is an appropriate choice.
Reference:
American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
Reference:
American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
Question 73 |
PG is a 86 YOW, weight 182 pounds, height 5’10”. Past medical history of hypertension, GI bleed, osteoarthritis, renal failure stage 4 (GFR = 15-30 mL/min), CHF with preserved ejection fraction. Her BP is 142/ 92, A1c 9.3. Her current Metformin 500mg by mouth BID, Insulin glargine 20 units SQ at bedtime, Atorvastatin 20mg by mouth daily, Lisinopril 5mg by mouth daily, Diltiazem 360mg daily, pantoprazole 40mg BID, Acetaminophen 650mg q6hr.
What should be PG’s goal A1c?
6.5
| |
7.5
| |
8.0 | |
8.5 |
Question 73 Explanation:
The patients A1C goal should be <8 because they have multiple chronic illnesses of HTN, CKD stage 4, osteoarthritis, and heart failure and they are elderly. The patient does not have end stage chronic illness that meets the <8.5 criteria. The <7.5% goal is solely due to age >65 years. The <7% goal is for non, elderly, healthy adults per ADA. The goal <6.5 is only for healthy, non elderly adults per AACE/ACE.
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Question 74 |
In a cohort study of 47,363 male US health professionals, the Health Professionals Follow-up Study (HPFS), regular aspirin use (≥2 times/week) found (RR, 0.79; 95% CI, 0.69–0.90) for colorectal cancer over 18 years of follow-up. How can this data best be interpreted?
I) Those who takes aspirin ≥2 times/week have 0.79 times the risk of colorectal cancer
II) Those who takes aspirin ≥2 times/week have 0.21 times the risk of colorectal cancer
III) Those who takes aspirin ≥2 times/week have 21% lower risk of colorectal cancer
IV) Those who takes aspirin ≥2 times/week have 79% lower risk of colorectal cancer
II
| |
II and III
| |
I and IV
| |
I and III
|
Question 74 Explanation:
Relative risk can be stated as 0.79 times as likely or 0.79 times the risk, but it could also be illustrated as a relative risk reduction and stated as a 21% risk reduction or 21% lower risk by taking the medication.
Reference:
I. Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/ II. Confidence Intervals for the Risk Ratio (Relative Risk). (n.d.) Retrieved Jan. 24, 2017 from: http://sphweb.bumc.bu.edu/otlt/mph-modules/bs/bs704_confidence_intervals/bs704_confidence_intervals8.html
Reference:
I. Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/ II. Confidence Intervals for the Risk Ratio (Relative Risk). (n.d.) Retrieved Jan. 24, 2017 from: http://sphweb.bumc.bu.edu/otlt/mph-modules/bs/bs704_confidence_intervals/bs704_confidence_intervals8.html
Question 75 |
WM did not receive influenza vaccine prior to the start of this season, it’s now December. He did get influenza vaccine last year. Which of the following is correct course of action
Skip influenza vaccine for this year since it’s too late.
| |
Skip influenza vaccine for this year since he received vaccine last year.
| |
Start WM on Tamiflu to prevent him from getting influenza.
| |
Vaccinate him with influenza vaccine since influenza season lasts until March in your community. |
Question 75 Explanation:
Influenza vaccine is recommended annually, thus, WM should not skip it this year, and B is incorrect. Also, per the CDC, seasonal influenza outbreaks can occur as early as October, however, most activity peaks in January or later. Thus, it is not too late for WM to receive his vaccine in December, thus A is incorrect. Lastly, antiviral medications such as Tamiflu are an important adjunct to vaccinations. They are recommended as early as possible for any patient with confirmed or suspected influenza who, is 1) Hospitalized, 2) has severe, complicated, or progressive illness or 3) is at higher risk for influenza complications. Thus, WM is not a candidate with the given information and C is incorrect.
Reference:
Key Facts About Seasonal Flu Vaccine. Centers for Disease Control and Prevention. 2016. Available at: http://www.cdc.gov/flu/protect/keyfacts.htm. Accessed September 27, 2016.
Reference:
Key Facts About Seasonal Flu Vaccine. Centers for Disease Control and Prevention. 2016. Available at: http://www.cdc.gov/flu/protect/keyfacts.htm. Accessed September 27, 2016.
Question 76 |
In the US Nurses’ Health Study (NHS) cohort study, where they looked at association of regular aspirin use (≥two 325 mg tablets/week) and colorectal cancer in 82,911 women found (RR, 0.77; 95% CI, 0.67–0.88) over 20 years of follow-up. In an another analysis of the NHS, regular aspirin use, investigator also found (hazard ratio [HR]=0.72, 95% CI 0.56–0.92), what does this say about the mortality from colorectal cancer?
How can this data best be interpreted?
Those who takes aspirin ≥2 times/week have 23% lower risk of colorectal cancer
| |
Those who takes aspirin ≥2 times/week have 0.77% lower risk of colorectal cancer
| |
Those who takes aspirin ≥2 times/week have 28% lower risk of colorectal cancer
| |
Those who takes aspirin ≥2 times/week have 23% reduction in death from colorectal cancer |
Question 76 Explanation:
Relative risk can be stated as 0.77 times as likely or 0.77 times the risk, but it could also be illustrated as a relative risk reduction and stated as a 23% risk reduction or 23% lower risk by taking the medication.
Reference:
Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/
Reference:
Irwig, Les. Chapter 18: Relative risk, relative and absolute risk reduction, number needed to treat and confidence intervals. Smart health choices: making sense of health advice. Judy Irwig, 2007. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/books/NBK63647/
Question 77 |
In the US Nurses’ Health Study (NHS) cohort study, where they looked at association of regular aspirin use (≥two 325 mg tablets/week) and colorectal cancer in 82,911 women found (RR, 0.77; 95% CI, 0.67–0.88) over 20 years of follow-up. In an another analysis of the NHS, regular aspirin use, investigator also found (hazard ratio [HR]=0.72, 95% CI 0.56–0.92), what does this say about the mortality from colorectal cancer? How can this data best be interpreted?
Those who takes aspirin regularly have 72% lower risk of colorectal cancer
| |
Those who takes aspirin regularly have 28% reduction in death from colorectal cancer
| |
Those who takes aspirin regularly have 0.23% lower risk of colorectal cancer
| |
Those who takes aspirin regularly have 77% lower risk of colorectal cancer |
Question 77 Explanation:
Hazard ratio can be used to compare time-to-event data between 2 groups. In this case the time to event was 20 years-to-death from colorectal cancer and the groups were patients taking aspirin 325mg 2 or more times a week and patients that did not. With the HR being 0.72, the patients taking the aspirin were 0.72 times likely to die at any time during the 20 years. This means that aspirin had a 28% reduction in death from colorectal cancer, 1 – 0.72 = 0.28.
Reference:
Sedgwick, Philip, and Katherine Joekes. "Interpreting hazard ratios." BMJ: British Medical Journal 351 (2015).
Reference:
Sedgwick, Philip, and Katherine Joekes. "Interpreting hazard ratios." BMJ: British Medical Journal 351 (2015).
Question 78 |
JM is a 72 YOM who comes to the ER with gastroenteritis. After reviewing his vaccination records you find that he has received 1 dose of Tdap when he was 60 years old, had influenza vaccine and PPSV23 3 years ago when he was admitted in the hospital for exacerbation of HF. It is Oct 2016, what vaccine should JM receive?
Influenza
| |
PCV13 and Influenza
| |
Influenza, PCV13, Zoster and Td booster
| |
Influenza, PCV13, Zoster, Td booster and MMR |
Question 78 Explanation:
Influenza vaccine is recommended annually, thus JM is a candidate, as he hasn’t received it since 2013. Patient is also a candidate for the herpes zoster vaccine as he is over the age of 60. A Tdap booster is recommended every 10 years, thus JM is a candidate as his last Tdap was 12 years ago. Lastly, patient is a candidate for the PCV13 vaccine as it is recommend 1 or more years after PPSV23 shot (given 3 yeas ago.) Patient is not a candidate for MMR, as individuals, who have been born prior to 1957 are considered immune to measles and mumps (patient born in 1944.)
Reference:
Adult Immunization Schedule. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated April 20, 2016. Accessed September 5, 2016
Reference:
Adult Immunization Schedule. Centers for Disease Control and Prevention. http://www.cdc.gov/vaccines/schedules/hcp/adult.html. Updated April 20, 2016. Accessed September 5, 2016
Question 79 |
Which of the following would be most appropriate to treat stenotrophomonas maltophilia?
Meropenem
| |
Vancomycin
| |
Ciprofloxacin
| |
Sulfamethoxazole/trimethoprim |
Question 79 Explanation:
Primary treatment for stenotrophomonas maltophilia is SMX-TMP. Meropenem, ciprofloxacin, and vancomycin have no coverage.
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Reference:
Gilbert D. The Sanford Guide to Antimicrobial Therapy 2014. Sperryville, Va.: Antimicrobial Therapy; 2014
Question 80 |
The rate that an outcome will occur given a particular exposure, compared to the rate of the outcome occurring in the absence of that exposure is definition of which of the following?
Incidence rate
| |
Prevelance rate
| |
Odds ratio
| |
Relative risk |
Question 80 Explanation:
RR = rate of an outcome occurring in an exposed group (treatment group/intervention group) divided by the rate of an outcome occurring in an unexposed group (control group)
Ex: Relative Risk = Rate of UTI in patients taking drug XYZ / rate of UTI in patients not on drug XYZ
Reference:
2x2 Contingency Table with Odds Ratios, etc. (n.d.). Retrieved Jan. 24, 2017 from: http://www.vassarstats.net/odds2x2.html
Ex: Relative Risk = Rate of UTI in patients taking drug XYZ / rate of UTI in patients not on drug XYZ
Reference:
2x2 Contingency Table with Odds Ratios, etc. (n.d.). Retrieved Jan. 24, 2017 from: http://www.vassarstats.net/odds2x2.html
Question 81 |
JK is a 67 years African American man who presents to your clinic for his blood pressure management. His past medical history includes Peptic ulcer disease and hypertension. His two BP readings are 160/98, 159/96 and HR 85. He says he has been adherent to his medication and lifestyle. He currently takes 12.5mg Chlorthalidone and Prilosec 20mg daily. Which of the following is the best strategy to manage his blood pressure?
Increase chlorthalidone to 25mg daily
| |
Add Norvasc 2.5 daily
| |
Add Lisinopril 5mg daily
| |
Strategies A or B could be used |
Question 81 Explanation:
As the patient is over the age of 60 and he does not have CKD or diabetes, his goal BP should be SBP < 150 mmHg or DBP < 90 mmHg, and he is not currently at this goal with his medication regimen. Options are to maximize the current medication dosage (option A), or to add a second agent. Since calcium channel blockers like Norvasc are recommended as initial treatment options in African Americans, choosing Norvasc over lisinopril would probably be the more effective option.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Question 82 |
Results from a Meta-analysis where they looked at frequency of postoperative arterial fibrillation in patients on Ascorbic acid after cardiac surgery found odds ratio, 0.44 (95% CI, 0.32 to 0.61). How can you interpret this data?
Ascorbic acid increased frequency of postoperative arterial fibrillation after cardiac surgery by 44%
| |
Ascorbic acid decreased frequency of postoperative arterial fibrillation after cardiac surgery by 44%
| |
There was no statistically significant difference in frequency of postoperative arterial fibrillation after cardiac surgery
| |
Ascorbic acid decreased frequency of postoperative arterial fibrillation after cardiac surgery by 56% |
Question 82 Explanation:
Odds ratio of 0.44 (44%) means that this group was associated with an event happening 44% of the time, compared to 1 (an event happening 100% of the time if unexposed), therefore 100 - 44 = 56%, which is the reduction caused by the exposure. Exposure is the use of ascorbic acid.
Reference:
Davies, Huw Talfryn Oakley, Iain Kinloch Crombie, and Manouche Tavakoli. "When can odds ratios mislead?." Bmj 316.7136 (1998): 989-991. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1112884/
Reference:
Davies, Huw Talfryn Oakley, Iain Kinloch Crombie, and Manouche Tavakoli. "When can odds ratios mislead?." Bmj 316.7136 (1998): 989-991. Retrieved Jan. 24, 2017 from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1112884/
Question 83 |
The Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society recommends covering what bacteria empirically for suspected VAP?
S. aureus and Pseudomonas aeruginosa
| |
Streptococcus and Pseudomonas aeruginosa
| |
Pseudomonas aeruginosa and ESBL
| |
S. aureus plus Streptococcus |
Question 83 Explanation:
These bacteria are some of the ones most commonly associated with VAP in the United States. This is based on surveillance data. They are also some of the most frequent isolates identified in international surveillance programs. Therefore, the guidelines recommend treatment to cover these bacteria.
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Question 84 |
PW is a 46 year African American man with a history of Chronic Kidney Disease due to radiocontrast media. His two average BP readings are 157/94 mm Hg, HR is 65. His CBC and CMP are within normal limits, except serum creatinine is 1.6. Which of the following is the best way to manage her hypertension according to the Eight Joint National Committee (JNC 8)?
Lifestyle modification
| |
Lifestyle modification and lisinopril 2.5mg daily
| |
Lifestyle modification and amlodipine 2.5mg daily
| |
Life style modification and metoprolol succinate 25md daily |
Question 84 Explanation:
The patient is less than 60 years old, African American, and has CKD. Therefore, his goal BP should be SBP < 140 mmHg and DBP < 90 mmHg. Option B is not the best choice because ACE inhibitors like lisinopril can worsen serum creatinine, and this patient already has a high serum creatinine. His heart rate is on the lower end of the normal range of 60-80, so adding metoprolol succinate would not be an ideal option. The best option is C.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Question 85 |
Number of new cases per population at risk in a given time period is a definition of which of the following?
Incidence rate
| |
Prevalence rate
| |
Mortality rate
| |
Odds ratio |
Question 85 Explanation:
Incidence rate = New reported cases / summed person-years of observation (avg population during time interval). Prevalence = Cases in a population in a given time period / total population at that time Mortality rate = deaths during specified time interval / population size at risk for death
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
Reference:
Dicker, R. C., Coronado, F., Koo, D., et al. Principals of Epidemiology in Public Health Practice, Third Edition: An Introduction to Applied Epidemiology and Biostatistics; Lesson 3, Section 2. Oct. 2006 Retrieved Jan. 24, 2017 from: https://www.cdc.gov/ophss/csels/dsepd/ss1978/lesson3/section2.html Updated: Nov. 2011
Question 86 |
KS is a 48 year old lady who presents to the ER with vertigo, nausea and vomiting after eating food from the previous night. She denies any focal numbness, tingling and weakness. She was having some unsteadiness and dizziness throughout the day. Her past medical history includes of multiple sclerosis, hypertension, diabetes, and hyperlipidemia. Her MS has been stable on glatiramer acetate for 7 years. What is the treatment of choice for MS exacerbation?
Methylprednisone 250mg IVPB daily for 4 days, followed by oral taper
| |
Methylprednisone 1gm IVPB daily for 5 days followed by oral taper
| |
Methylprednisone 250mg IVPB daily for 4 days
| |
Methylprednisone 1gm IVPB daily for 5 days |
Question 86 Explanation:
A literature review of management of MS exacerbation treatments concluded that IV steroids are the preferred route of administration. High doses of IV methylprednisolone varying from 500 to 1000 mg for 3-5 days has been found to be effective. Oral steroid tapers have no supporting evidence.
Reference:
Rae-Grant A, Ontaneda D. Management of acute exacerbations in multiple sclerosis. Ann Indian Acad Neurol. 2009;12(4):264. doi:10.4103/0972-2327.58283
Reference:
Rae-Grant A, Ontaneda D. Management of acute exacerbations in multiple sclerosis. Ann Indian Acad Neurol. 2009;12(4):264. doi:10.4103/0972-2327.58283
Question 87 |
Which of the following diagnostic lab test is recommended by the Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society in addition to clinical criteria to guide discontinuation of antibiotics?
Procalcitonin (PCT)
| |
C - Reactive protein (CRP)
| |
Modified Clinical Pulmonary Infection Score (CPIS)
| |
Clinical Criteria alone |
Question 87 Explanation:
The use of PCT levels can decrease antibiotic exposure without increasing treatment failure or mortality. As a result, costs are reduced as well as the occurrence of side effects. Current evidence does not support the use of CPIS to guide discontinuation of antibiotics since it is not reliable enough to determine whether antibiotic therapy should be continued or not. CRP was not mentioned in the guidelines as to whether it can be used to determine discontinuation of antibiotic therapy or not.
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Question 88 |
CJ is a 69 year old male with a history of diabetes, hypertension and hypercholesterolemia. His fasting lipid profile is TC 530 mg/dL; LDL-C 125; HDL-C 48 mg/dL; and TG 640 mg/dL. His A1c 8.1, calculate creatinine clearance is 65mls/hr, BP 135/80 mm Hg, HR 70 beats /min. His current medications includes metformin 1000mg po bid, lisinopril 20mg daily, sitagliptin 50mg bid and atorvastatin 20mg daily. What is the best pharmacological agent to initiate on CJ?
Increase atorvastatin to 80mg
| |
Niacin 500mg twice daily
| |
Fenofibrate 162mg daily
| |
Gemfibrozil 600mg twice daily |
Question 88 Explanation:
It is reasonable to add triglyceride-lowering medications such as fibrates or niacin to prevent pancreatitis in those with triglyceride levels >500 mg/dL, which applies to this patient as his TG level is 640 mg/dL. Answer C. is wrong because gemfibrozil should not be initiated in patients on statin therapy because of an increased risk for muscle symptoms and rhabdomyolysis. Fenofibrate may be considered concomitantly with a low- or moderate- intensity statin when triglycerides are above 500 mg/dL. For niacin, the IR dose should start at 100 mg TID and niacin does not lower triglyceride levels as much as fibrate do. Fenofibrates are dose adjusted for renal function. The best option is fenofibrate 162 mg daily, but this needs to be monitored for any symptoms of muscle pain exhibited by the patient, especially as the patient is at a higher risk due to being a diabetic.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1 Miller M, Stone N, Ballantyne C et al. Triglycerides and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2011;123(20):2292-2333. doi:10.1161/cir.0b013e3182160726.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1 Miller M, Stone N, Ballantyne C et al. Triglycerides and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2011;123(20):2292-2333. doi:10.1161/cir.0b013e3182160726.
Question 89 |
SJ is a 71 YOM, weight 253 pounds, height 5’ 11”. Past medical history gout, hypertension, dyslipidemia, COPD and pancreatitis while on Sitagliptin. His BP is 138/88, A1c is 9.4. Serum creatinine 1.0mg/dL. His current medications includes, Metformin 1000mg BID, Insulin glargine 30 units SQ at bedtime, Acarbose 100mg tid, Atorvastatin 80mg by mouth daily, Ramipril 10mg by mouth daily, Tiotropium 18mcg inhaled daily. Which of the following would be the most appropriate option for management of his type 2 diabetes Mellitus?
Add Empagliflozin 10mg by mouth daily
| |
Add Exenatide 2mg SQ once weekly
| |
Add Linagliptin 5mg by mouth daily
| |
Increase Insulin glargine 60 units and add Insulin Lispro sliding scale |
Question 89 Explanation:
Empagliflozin is the best option for this patient. Linagliptin is not an option since patient has already tried Sitagliptin (in the same drug class), and patient had pancreatitis. GLP1- agonists also are associated with pancreatitis so use of Exenatide would not be recommended. Pioglitazone should not be used because the patient is ~52% overweight and it can cause weight gain. Increasing the long acting insulin dose and adding short acting sliding scale is an not an appropriate option since sliding scale in elderly adults in on the BEERs list due to potential increased risk of errors/hypoglycemia.
Reference:
I. ADA 2016 Food and Drug Administration (US FDA) Drug Medwatch-FDA investigating reports of possible increased risk of pancreatitis and pre-cancerous findings of the pancreas from incretin mimetic drugs for type 2 diabetes. Retrieved Mar. 14, 2013. Available on the World Wide Web at http://www.fda.gov/Drugs/DrugSafety/ucm343187.htm. II. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 63:2227-2246, 2015.
Reference:
I. ADA 2016 Food and Drug Administration (US FDA) Drug Medwatch-FDA investigating reports of possible increased risk of pancreatitis and pre-cancerous findings of the pancreas from incretin mimetic drugs for type 2 diabetes. Retrieved Mar. 14, 2013. Available on the World Wide Web at http://www.fda.gov/Drugs/DrugSafety/ucm343187.htm. II. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 63:2227-2246, 2015.
Question 90 |
If 70 % of S. aureus isolate in your ICU are methicillin resistance, what anti-staphylococcus antibiotic should you use to treat suspected VAP?
piperacillin-tazobactam
| |
Oxacillin
| |
Vancomycin
| |
Moxifloxacin |
Question 90 Explanation:
Since there is 70% of S. aureus isolate in the ICU that is methicillin resistant, vancomycin would be indicated. Oxacillin and piperacillin-tazobactam has no MRSA activity. Moxifloxacin has some MRSA activity, but is not recommended to be used in VAP. Moxifloxacin may be used for community acquired MRSA pneumonia MRSA with lower MIC.
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Reference:
Kalil AC, Metersky ML, Klompas M, et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin Infect Dis. 2016;ciw353. doi:10.1093/cid/ciw353. Retrieved on feb 8th, 2017 from : https://academic.oup.com/cid/article/63/5/e61/2237650/Management-of-Adults-With-Hospital-acquired-and
Question 91 |
All of the following may increase triglycerides except?
Protease inhibitor
| |
Bile acid sequestrants
| |
Fish Oil
| |
Oral estrogens |
Question 91 Explanation:
Agents that can cause elevated triglycerides: oral estrogens, glucocorticoids, bile acid sequestrants, protease inhibitors, retinoic acid, anabolic steroids, sirolimus, raloxifene, tamoxifen, beta blockers (not carvedilol), and thiazides.
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Reference:
Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
Question 92 |
SR is a 69 YOM, weight 236 pounds, height 5’8”. Past medical history includes hypertension, diabetes mellitus, CHF with reduced ejection fraction. His BP 137/86, A1c 9.7, Serum creatinine 1.0 mg/dL. His current medications include Metformin 1000mg by mouth BID, Insulin glargine 20 units SQ at bedtime, Glipizide 10mg by mouth twice daily. Atorvastatin 40mg by mouth daily, Lisinopril 20mg by mouth daily, Carvedilol 12.5mg BID, Furosemide 20mg by mouth daily and Spironolactone 12.5mg by mouth daily. SR also complains of several hypoglycemic episodes on days he skips meal or eats late.
Which of the following would be the most appropriate option for management of his type 2 diabetes Mellitus?
D/C Glipizide and add Pioglitazone 30mg by mouth daily
| |
D/C Glipizide and add Dapagliflozin 10mg by mouth daily
| |
D/C Glipizide and add Dulaglutide 0.75mg SQ once weekly
| |
Increase Insulin glargine 40 units and add Insulin Lispro sliding scale |
Question 92 Explanation:
Glipizide should be discontinued because it works by increasing insulin secretion and one of its main side effects is hypoglycemia. Since the patient does not eat stable meals, this is what is contributing to his episodes of hypoglycemia and this drug should not be used for him. Pioglitazone is not a good option for this patient since there is a black box warning for exacerbating heart failure. Dapagliflozin is not a good option since it works by reducing reabsorption in the kidney which can cause volume depletion in this patient who is already on furosemide. Adding Dulaglutide 0.75mg once weekly would simplify regimen and drop A1c to goal. GLP-1 agonist can drop A1c by average 1%-1.5%. Option D is not ideal either because increasing a long acting insulin glargine in addition to sliding scale will just contribute to hypoglycemia. Sliding scale insulin are potentially inappropriate medication per the beer’s criteria. IBW = 68.4 kg; actual BW = 107.3 kg. >120% overweight; adjBW = 84 kg, CrCL = 82.8 mL/min
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Question 93 |
SR is a 69 YOM, weight 236 pounds, height 5’8”. Past medical history includes hypertension, diabetes mellitus, CHF with reduced ejection fraction. His BP 137/86, A1c 9.7, Serum creatinine 1.0 mg/dL. His current medications include Metformin 1000mg by mouth BID, Insulin glargine 20 units SQ at bedtime, Glipizide 10mg by mouth twice daily. Atorvastatin 40mg by mouth daily, Lisinopril 20mg by mouth daily, Carvedilol 12.5mg BID, Furosemide 20mg by mouth daily and Spironolactone 12.5mg by mouth daily. SR also complains of several hypoglycemic episodes on days he skips meal or eats late.
What should be SR’s goal A1c?
<6.5
| |
<7.0
| |
<7.5
| |
<8.5 |
Question 93 Explanation:
This patient is elderly >65 years old which qualifies him for A1C goal <7.5%. While they do have certain co-morbidities/chronic illnesses of CHF, stage 2 CKD (CrCl 82.8 mL/min), and HTN, this patient does not meet at least 3 chronic illnesses that meet the criteria per the guidelines to have a less stringent A1C goal of <8. This list consists of “arthritis, cancer, congestive heart failure, depression, emphysema, falls, hypertension, incontinence, stage 3 or worse chronic kidney disease, myocardial infarction, and stroke”. This patient only meets 2 of these. In order to meet goal for <8.5 goal A1C, the patient must qualify with presence of one of the following: “single end-stage chronic illness, such as stage 3–4 congestive heart failure or oxygen-dependent lung disease, chronic kidney disease requiring dialysis, or uncontrolled metastatic cancer”. The goal <6.5 is only for healthy, nonelderly adults per AACE/ACE.
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Reference:
I. American Diabetes Association. In Standards of Medical Care in Diabetes 2016. Diabetes Care 2016;39(Suppl. 1) Avaiable at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf
II. Garber AJ, et al. Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm – 2016 Executive Summary. Endocr Pract. 2016; 22(1):84-113. Retrieved on Feb 8th, 2017 from : http://journals.aace.com/doi/10.4158/EP151126.CS
Question 94 |
Marked limitation of physical activity, comfortable at rest, but ordinary physical activity results in symptoms of HF. What stage of NYHA functional classification?
Stage C
| |
Stage D
| |
Class III
| |
Class IV |
Question 94 Explanation:
The guidelines state that class III is defined as an individual who has marked limitation of physical activity, comfortable at rest, but ordinary physical activity results in symptoms of HF. Class IV is defined as an individual who is unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest. Stages A-D are not NYHA functional classification. Stage D is when an individual has refractory HF that requires specialized interventions, and Stage C is when there is structural heart disease with prior or current symptoms of HF.
Reference
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Reference
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Question 95 |
Which of the following medications are known to prevent heart failure in patients with myocardial infarction (MI)?
Statin
| |
Angiotensin-converting enzyme (ACE) Inhibitor or angiotensin-receptor blocker (ARB)
| |
Evidence-Based Beta Blocker example Bisoprolol, metoprolol succinate and Carvedilol
| |
All of the Above are known to prevent Heart failure in patient with MI |
Question 95 Explanation:
All of the above are known to prevent heart failure in patients with MI. The guidelines state that in all patients with a recent or remote history of MI or ACS, statins should be used to prevent symptomatic HF and cardiovascular events. Those with known atherosclerotic disease are more likely to develop HF. Therefore, aggressive treatment with statins can help to reduce the likelihood of HF in at-risk patients. The guidelines also state that in all patients with a recent or remote history of MI or ACS and reduced EF, ACE inhibitors should be used to prevent symptomatic HF and reduce mortality. ARBs would be appropriate if patients are intolerant to ACE inhibitors. This can also be applied to beta-blockers. Patients with a recent or remote history of MI or ACS and reduced EF should use evidence-based beta-blockers to reduce mortality. In addition, ACE inhibitors and beta-blockers should be used in all patients with a reduced EF to prevent symptomatic HF, even if they do not have a history of MI.
Reference
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Reference
Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol. 2013;62(16):e147-e239. doi:10.1016/j.jacc.2013.05.019. Retirved on Feb 6th from : http://circ.ahajournals.org/content/128/16/e240
Question 96 |
In a study where the investigators measured decrease in weight in 120 patients after 90 days of initiating this hypothetical drug, the mean decrease in weight was 16 pounds with standard error of mean 4.2 pounds, what is the 95% confidence interval for the decrease in weight with this drug? What is the Interpretation of this Confidence interval?
8.23-24.23pounds
| |
11.8-27.8pounds
| |
9.5-26.5pounds
| |
12.4-18.4 pouds |
Question 96 Explanation:
16 + (1.96 x 4.2) = 24.23pounds.
16 - (1.96 x 4.2) = 8.23pounds.
The 95% confidence interval is from 8.23 pounds to 24.23pounds, which means we can be 95% sure that the mean decrease in weight after initiating the drug falls within this range. You can also say that there is a 5% chance that the mean decrease in weight of the population falls outside of this range.
Reference:
"Statistics At Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
16 - (1.96 x 4.2) = 8.23pounds.
The 95% confidence interval is from 8.23 pounds to 24.23pounds, which means we can be 95% sure that the mean decrease in weight after initiating the drug falls within this range. You can also say that there is a 5% chance that the mean decrease in weight of the population falls outside of this range.
Reference:
"Statistics At Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 97 |
Which of the following is dichotomous variable?
Sex
| |
Pain yes/ Pain no
| |
alive / dead
| |
A, B and C. |
Question 97 Explanation:
Dichotomous data is considered categorical data that only has two categories, or two answer choices. All 3 answer choices have only 2 categories: sex has male or female, pain is yes or no, and alive or dead is only two options also.
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Question 98 |
A 37 years old caucasian man with no past medical history presents to your clinic. His two average BP reading is 146/87 mm Hg, HR is 65. His CBC and CMP are within normal limits. Which of the following is the best way to manage her hypertension according to the Eight Joint National Committee (JNC 8)?
Lifestyle modification only
| |
Lifestyle modification and amlodipine 2.5mg daily
| |
Life style modification and hydrochlorothiazide 25mg daily
| |
B or C, both are appropriate |
Question 98 Explanation:
The patient is under the age of 60 and is considered a member of the general population since there is no known history, and he is Caucasian. JNC8 does not address definitions of hypertension and prehypertension, but defines the threshold for initiating pharmacologic therapy. Medications should be started when SBP is 140 mmHg or higher. For Caucasian patients, either a thiazide-type diuretic, an ACEI or ARB, or a CCB should be initiated. Both choices B and C are appropriate options at appropriate starting doses.
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Reference:
James P, Oparil S, Carter B et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults. JAMA. 2014;311(5):507. doi:10.1001/jama.2013.284427. Retrieved Jan. 24, 2017 from: http://jamanetwork.com/journals/jama/fullarticle/1791497
Question 99 |
LM is a 62 years old male with a new diagnosis of diabetes. His past medical history includes hypertension for which he takes amlodipine 5mg daily and hydrochlorothiazide25mg daily. His cholesterol panel includes total cholesterol (TC) 222 mg/dL, low-density lipoprotein cholesterol (LDL-C) 105 mg/dL, triglycerides (TG) 330 mg/dL, and high-density lipoprotein cholesterol (HDL-C) 51 mg/dL. His vital signs include BP 125/75 mm Hg and HR 70 beats/minute. His physician put him on metformin 500mg by mouth twice daily. Besides metformin what is the other pharmacologic regimen that should be started on LM?
Atorvastatin 80mg daily
| |
Rosuvastatin 10mg daily
| |
Gemfibrozil 600mg twice daily
| |
Simvastatin 40mg daily |
Question 99 Explanation:
This patients has diabetes, age between 40 and 75 years, and has an LDL between 70 and 189 mg/dL , which places him in one of the four statin benefit groups. These characteristics also warrant using the Pooled Cohort Risk Assessment Equation to estimate his 10-year ASCVD risk. Using the ASCVD Risk Estimator, and assuming he is a nonsmoker and is Caucasian, his 10-year ASCVD risk is 22.1%. Since it is greater than 7.5%, he should receive a high intensity statin therapy. Rosuvastatin 10 mg and Simvastatin 40 mg are considered moderate-intensity statin therapies, and gemfibrozil is not a statin. A is the best option because Atorvastatin 80 mg is high intensity statin therapy.
Reference:
I. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
II. ASCVD Risk Estimator. Tools.acc.org. 2016. Available at: http://tools.acc.org/ASCVD-Risk-Estimator/ . Accessed June 8, 2016.
Reference:
I. Stone N, Robinson J, Lichtenstein A et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults. Circulation. 2013;129(25 suppl 2):S1-S45. doi:10.1161/01.cir.0000437738.63853.7a. Retrieved on Feb 6th 2017 from : http://circ.ahajournals.org/content/129/25_suppl_2/S1
II. ASCVD Risk Estimator. Tools.acc.org. 2016. Available at: http://tools.acc.org/ASCVD-Risk-Estimator/ . Accessed June 8, 2016.
Question 100 |
In a publication observed mean weight of 200 patients was reported as 69.4 ±9.3 kg. If 9.3 kg is the SD, calculate the SEM?
60.1kg
| |
0.658kg
| |
9.3kg
| |
17.94kg
|
Question 100 Explanation:
SEM = SD/square root of n.
SEM = 9.3 /square root of 200.
= 0.658 kg
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
SEM = 9.3 /square root of 200.
= 0.658 kg
Reference:
"Statistics at Square One | The BMJ". Bmj.com. 2016. Web. 7 Nov. 2016. Available at: http://www.bmj.com/about-bmj/resources-readers/publications/statistics-square-one
Once you are finished, click the button below. Any items you have not completed will be marked incorrect.
There are 100 questions to complete.
|
List |

Comments are closed.