CGP
- Cardiovascular
- Endocrine
- Geriatrics
- Gastrointestinal disorder
- Infectious disease
- Men’s and women’s health
- Neurology
- Oncology
- Ophthalmic and otics
- Pain management
- Psychiatric
- Renal disease / fluids & electrolytes
- Respiratory
- Skin conditions
- Pharmacokinetics-Pharmacodynamics
- Biostatistics and pharmacoeconomics
- Pharmacy policy, procedure and regulations
The questions in this section are intended to test your knowledge and skills on Geriatric Pharmacy including biostatistics for practicing pharmacist and pharmacist preparing for CGP (Board Certified Geriatric Pharmacist).
Click on the right arrow to go to the next question. If the arrow is missing hover your mouse to the lower right, above the ad until the mouse is clickable.
BCPS | Pharmacokinetics pharmacodynamics
Congratulations - you have completed BCPS | Pharmacokinetics pharmacodynamics.
You scored %%SCORE%% out of %%TOTAL%%.
Your performance has been rated as %%RATING%%
Your answers are highlighted below.
Question 1 |
Which of the following is true?
Acidic drugs are highly protein bound therefore have high volume of distribution. | |
Acidic drugs are less protein bound therefore have low volume of distribution. | |
Acidic drugs are highly protein bound therefore have low volume of distribution | |
Acidic drugs are less protein bound therefore have high volume of distribution |
Question 1 Explanation:
Acidic drugs are primarily bind to albumin (highly protein bound). Drugs that are highly protein/plasma bound tend to stay in the blood longer, resulting in a lower volume of distribution. Drugs that primarily distribute into tissue have a high volume of distribution.
Question 2 |
Which of the following is true?
Basic drugs are highly protein bound therefore have high volume of distribution. | |
Basic drugs are less protein bound therefore have low volume of distribution | |
Basic drugs are highly protein bound therefore have low volume of distribution | |
Basic drugs are less protein bound therefore have high volume of distribution |
Question 2 Explanation:
Basic drugs are less protein bound and therefore readily distribute into tissue, resulting in a higher volume of distribution. These drugs often stay for longer periods of time in organs and tissues, often leading to higher concentrations, narrower therapeutic index and decreased clearance.
Question 3 |
If a 75 Kg patient is given 1.5 gm of vancomycin what is the excepted maximum blood concentration (Cmax) if Vd of 0.9L/kg is used?
25.6 mg/L | |
22.2 mg/mL | |
15.3 mg/mL | |
26.1 mg/mL |
Question 3 Explanation:
C0 = Dose/Vd
C0 = 1500mg/67.5L = 22.2 mg/L
Question 4 |
Which of the following statements best describes piperacillin/tazobactam’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 4 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 5 |
Which of the following statements best describes Levofloxacin’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 5 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 6 |
Administration of 25mg of a XYZ drug intravenously and 100mg XYZ drug orally revealed the same area under the curve. What is the bioavailability of the oral drug?
100% | |
75% | |
50% | |
25% |
Question 6 Explanation:
F = (AUC PO)/(AUC IV) x (Dose IV)/(Dose PO)
F = 1/1 x 25/100 = 0.25 X 100% = 25%
Question 7 |
Which of the following statements best describes Tigecycline’s pharmacodynamics property?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 7 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, tigecycline, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, tigecycline, vancomycin.
Question 8 |
Volume of Distribution of Levetiracetam is 0.7 L/kg, what would be the maximum blood concentration (Cmax) following infusion of a 1gm IVB on a patient that weighs 35kg.
32.4 mg/L | |
40.8 mg/L | |
37.2 mg/L | |
55.9 mg/L |
Question 8 Explanation:
Cmax = Dose/Vd
Cmax = 1000mg/24.5L = 40.8 mg/L
Question 9 |
Volume of Distribution of Levetiracetam is 0.7 L/kg, what would be the maximum blood concentration (Cmax) following infusion of a 1gm IVB on a patient that weighs 35kg.
If the Half-life of the Levetiracetam is 5 hrs, what is the expected blood Levetiracetam concentration after 12hrs? (Cmax = 40.8 mg/L)
6.2 mg/L | |
5.8 mg/L | |
6.8mg/L | |
7.6 mg/L |
Question 9 Explanation:
Ke = 0.693/(t1/2 ) = 0.14 h-1
C = Cmax x e-ke x t = 40.8 x e-0.14 x 12 = 7.6 mg/L
Question 10 |
CL is a 44-year-old female admitted in hospital with UTI and C. Difficle infection. Her weight is 88 kg. She has a normal renal function. Patient is allergic to quinolones. She is currently on Cefepime 2gm IV every 12 hours, Metronidazole 500mg IV every 6 hours and Vancomycin PO 250mg four times daily. Two days later the blood culture was positive for Pseudomonas Aeruginosa with following sensitivity and MIC:
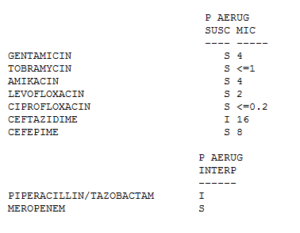 The volume of distribution of Cefepime is 18 L. After a 30-minute infusion of Cefepime what is the drug blood concentration? Round to the nearest whole number.
The volume of distribution of Cefepime is 18 L. After a 30-minute infusion of Cefepime what is the drug blood concentration? Round to the nearest whole number.
The volume of distribution of Cefepime is 18 L. After a 30-minute infusion of Cefepime what is the drug blood concentration? Round to the nearest whole number. 111 mg/L | |
252 mg/L | |
193 mg/L | |
222 mg/L |
Question 10 Explanation:
C0 = Dose/Vd = 2000mg/18L= 111 mg/L
Question 11 |
CL is a 44-year-old female admitted in hospital with UTI and C. Difficle infection. Her weight is 88 kg. She has a normal renal function. Patient is allergic to quinolones. She is currently on Cefepime 2gm IV every 12 hours, Metronidazole 500mg IV every 6 hours and Vancomycin PO 250mg four times daily. Two days later the blood culture was positive for Pseudomonas Aeruginosa with following sensitivity and MIC:
The volume of distribution of Cefepime is 18 L. The elimination half-life of Cefepime is 2 hours. Approximately after how many hours would the Cefepime blood concentration fall below MIC?
The volume of distribution of Cefepime is 18 L. The elimination half-life of Cefepime is 2 hours. Approximately after how many hours would the Cefepime blood concentration fall below MIC? 2 hours | |
4 hours | |
6 hours | |
8 hours |
Question 11 Explanation:
k= 0.693/(t1/2 )= = 0.693/(2 )= 0.345
Fraction remaining after 1 half life (2 hours) = e^(-kt)= e – 0.345 x 2= 0.50
Amount remaining after 1 half life (2 hours) = 0.50 x 111mg/mL = 55.5 mg/mL
Fraction remaining after 2 half lives (4 hours) = e^(-kt)= e – 0.345 x4 = 0.25
Amount remaining after 2 half lives (4 hours) = 0.25 x 111 mg/mL = 27.75 mg/mL
Fraction remaining after 3 half lives (6 hours) = e^(-kt)= e – 0.345 x6 = 0.125
Amount remaining after 3 half lives (6 hours) = 0.125 x 111 mg/mL = 13.875 mg/mL
Fraction remaining after 4 half lives (8 hours) = e^(-kt)= e – 0.345x8 = 0.0625
Amount remaining after 4 half lives (8 hours) = 0.0625 x 111 mg/mL = 6.93 mg/mL
It will take 4 half lives for cefepime to reach a concentration of 6.93 mg/mL Since the MIC of Cefepime is 8, it will take approximately 8 hours for cefepime to reach a concentration of 6.93 mg/mL, which is a blood concentration below MIC.
Fraction remaining after 1 half life (2 hours) = e^(-kt)= e – 0.345 x 2= 0.50
Amount remaining after 1 half life (2 hours) = 0.50 x 111mg/mL = 55.5 mg/mL
Fraction remaining after 2 half lives (4 hours) = e^(-kt)= e – 0.345 x4 = 0.25
Amount remaining after 2 half lives (4 hours) = 0.25 x 111 mg/mL = 27.75 mg/mL
Fraction remaining after 3 half lives (6 hours) = e^(-kt)= e – 0.345 x6 = 0.125
Amount remaining after 3 half lives (6 hours) = 0.125 x 111 mg/mL = 13.875 mg/mL
Fraction remaining after 4 half lives (8 hours) = e^(-kt)= e – 0.345x8 = 0.0625
Amount remaining after 4 half lives (8 hours) = 0.0625 x 111 mg/mL = 6.93 mg/mL
It will take 4 half lives for cefepime to reach a concentration of 6.93 mg/mL Since the MIC of Cefepime is 8, it will take approximately 8 hours for cefepime to reach a concentration of 6.93 mg/mL, which is a blood concentration below MIC.
Question 12 |
What is the T>MIC achieved by Cefepime 1gm IV every 12 hours? Vd of cefepime is 18L, half life is 2 hours, and MIC = 8.
70.5% | |
53.6% | |
46.7% | |
68.2% |
Question 12 Explanation:
T>MIC = ln ( Dose/(Vd x MIC) ) x (t1/2)/ln〖(2)〗 x 100/DI
T>MIC = ln ( (1000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 46.7%
T>MIC = ln ( (1000 mg)/(18 L x 8) ) x (2 hours)/ln〖(2)〗 x 100/(12 hours)
T>MIC = 46.7%
Question 13 |
What pharmacodynamics property is demonstrated by Metronidazole?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: Cmax/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: AUC/MIC |
Question 13 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 14 |
HN is a 29-year-old female who is the hospital with a cellulitis. Physician would like pharmacy to dose the vancomycin. She weighs 67kg, height 70 feet, creatinine clearance 120 mL/min. Calculate the population specific half-life. Use Vd of 0.7L/kg.
2.7 h | |
4.5 h | |
2.1 h | |
3.4 h |
Question 14 Explanation:
t1/2 = (0.693 x Vd)/CL
t1/2 = (0.693 x 700mL/kg x67kg)/(120mL/min)
= 270 minutes = 4.5 h
t1/2 = (0.693 x 700mL/kg x67kg)/(120mL/min)
= 270 minutes = 4.5 h
Question 15 |
You decide to give vancomycin 1gm IV every 8 hours. Vancomycin trough was 24.5 prior to the 5th dose. Vancomycin was held. 5 hours later another vancomycin level was ordered it came back 14.5. Calculate the patient specific half-life. Round to the nearest whole number.
8 h | |
12 h | |
5 h | |
7 h |
Question 15 Explanation:
Ke= ln〖C1-lnC2 〗/(t2-t1)
Ke= ln〖(24.5)-ln〖(14.5)〗 〗/(37-32) = 0.104
T1/2= 0.693/0.104 = 6.66 h = 7h
Ke= ln〖(24.5)-ln〖(14.5)〗 〗/(37-32) = 0.104
T1/2= 0.693/0.104 = 6.66 h = 7h
Question 16 |
After administration of 50mg of a drug intravenously and 100mg of the same drug orally revealed same drug blood concentration. What is the bioavailability of the oral drug?
40 % | |
20 % | |
80 % | |
50 % |
Question 16 Explanation:
F = (AUC PO)/(AUC IV) x (Dose IV)/(Dose PO)
F = 1/1 x 50/100 = 0.5 X 100% = 50%
F = 1/1 x 50/100 = 0.5 X 100% = 50%
Question 17 |
HT is a 56-year-old man who is being treated with tobramycin and oxacillin for his cellulitis. HT’s weight is 76 kg, height is 6’ 2”, Creatinine clearance 128mls/hr. After a 500mg dose of tobramycin his 9hrs random came back at 6.5 mg/L and 14hrs 1.2mg/L. Calculate the half-life and elimination rate constant.
0.34 h-1, 2.1 h | |
0.67 h-1, 1.03 h | |
0.28 h-1, 2.47 h | |
0.56 h-1, 1.23 h |
Question 17 Explanation:
Ke= ln〖C1-lnC2 〗/(t2-t1)
Ke= ln〖(6.5 mg/L)-ln〖(1.2 mg/L)〗 〗/((14-9) ) = 0.34 h-1
T1/2= 0.693/0.34 = 2.1 h
Ke= ln〖(6.5 mg/L)-ln〖(1.2 mg/L)〗 〗/((14-9) ) = 0.34 h-1
T1/2= 0.693/0.34 = 2.1 h
Question 18 |
What pharmacodynamics property is demonstrated by azithromycin?
Time-dependent killing, with minimal persistent effects: T>MIC | |
Time-dependent killing, with moderate prolonged persistent effects: AUC/MIC | |
Concentration-dependent killing with prolonged persistent effects: AUC/MIC, peak/MIC | |
Concentration dependent killing with persistent effects: peak/MIC |
Question 18 Explanation:
-T>MIC: the pharmacodynamics outcome that is correlated with efficacy for time dependent drugs; increased bacterial killing is based on the percentage of time the concentration exceeds the MIC. Drugs reach a saturable killing rate, therefore, increasing drug concentrations more will not affect the bacterial activity. Example of drugs: Penicillins, cephalosporings, monobactmas, clindamycin, macrolides, linezolid, tetracyclines.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
-Peak/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. The rate and extend of killing of bacteria will increase with increased drug concentrations relative to the MIC. Administer higher doses with a decreased frequency of administration. Examples of drugs: aminoglycosides, floroquinolones, ketolide, metronidazole, oritavancin.
-AUC/MIC: the pharmacodynamics outcome that is correlated with efficacy for concentration depend drugs. It measures the AUC relative to the MIC of the organisms. Administer higher doses with a decreased frequency of administration. Example of drugs: floroquinolones, macrolides, tetracyclines, vancomycin.
Question 19 |
SR is a 72 year old female admitted to ICU with PNA, A Fib, CHF with preserved left ventricular function. She weighs 76 kg. She has history of lung cancer for which she is being treated with cyberknife and chemotherapy as outpatient, history of hypertension, hyperlipidemia, hypothyroidism, COPD. On admission her WBC is 1.0 K/uL, bands of 32% and segs of 42%. SR was started on Vancomycin, Levofloxacin and Aztreonam for HAP. She is also on the electrolyte replacement protocol. She is allergic to PCN/cephalosporin (rash). For her A. Fib she was given Amiodarone 400mg orally BID and Diltiazem 10mg/hr. She also received few doses of furosemide for her CHF. What significant drug / drug interaction do you identify?
Furosemide and Amiodarone | |
Vancomycin and Amiodarone | |
Aztreonam and Amiodarone | |
Levofloxacin and Amiodarone |
Question 19 Explanation:
There is a drug interaction between levofloxacin and amiodarone, which may increase the risk of QT prolongation. Levofloxacin is associated with QT prolongation and rarely torsades de pointes. Amiodarone also has a risk of QT prolongation and torsades de pointes. This drug interaction is possible for days to weeks after amiodarone is discontinued because amiodarone has a long half-life. There is also a drug interaction with furosemide and amiodarone. Caution must be used because loop diuretics can lower potassium and magnesium levels, which can cause amiodarone to not work effectively, but patient is on electrolyte replacement protocol and on it for short duration.
Reference:
Gold Standard, Inc. Levofloxacin. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=746&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Gold Standard, Inc. Amiodarone. Clinical Pharmacology [database online]. Available at: https://www.clinicalpharmacology-ip.com/Forms/Monograph/monograph.aspx?cpnum=25&sec=moninte&t=0. Accessed: May 18, 2016.
Question 20 |
Which of the following cardiovascular changes is/are seen as body ages?
Increase in total peripheral resistance | |
Increase in cardiac output | |
Increase in baroreceptor sensitivity | |
Increase in Beta-adrenergic receptor sensitivity |
Question 20 Explanation:
Answer A. With aging, blood pressure and total peripheral resistance increase, however, a decrease in cardiac output is seen. A progressive decline in baroreceptor sensitivity is a characteristic feature of human aging as is a decrease in Beta-adrenergic receptor sensitivity.
Reference:
1. Martin WH 3rd e. Effects of aging, gender, and physical training on peripheral vascular function. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/1860209. Accessed October 12, 2016.
2. O'Mahony D e. Reduced baroreflex sensitivity in elderly humans is not due to efferent autonomic dysfunction. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/10600664. Accessed October 12, 2016.
3. Ferrara N, Komici K, Corbi G et al. β-adrenergic receptor responsiveness in aging heart and clinical implications. Frontiers in Physiology. 2014;4. doi:10.3389/fphys.2013.00396.
Reference:
1. Martin WH 3rd e. Effects of aging, gender, and physical training on peripheral vascular function. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/1860209. Accessed October 12, 2016.
2. O'Mahony D e. Reduced baroreflex sensitivity in elderly humans is not due to efferent autonomic dysfunction. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/10600664. Accessed October 12, 2016.
3. Ferrara N, Komici K, Corbi G et al. β-adrenergic receptor responsiveness in aging heart and clinical implications. Frontiers in Physiology. 2014;4. doi:10.3389/fphys.2013.00396.
Question 21 |
Which of the following renal changes does not occur as body ages?
Increase in total body water | |
Decrease in renal mass | |
Decrease in renal blood flow | |
Decrease Glomerular filtration rate |
Question 21 Explanation:
Answer: A. There is a progressive reduction in total body water and lean body mass that occurs and which results in a relative increase in body fat. Renal mass decreases with age and reflects the reduction in nephrons. Both renal plasma flow and as well as glomerular filtration rate decline with age.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Question 22 |
Which of the following pulmonary changes is/are seen as body ages?
Decrease in expiratory flow rate | |
Decrease in vital capacity | |
Decrease in respiratory muscle strength | |
All of the above changes are seen a body ages |
Question 22 Explanation:
Answer D. Expiratory flow rates decrease with aging and typically show changes in the flow-volume curves. Other age-related changes that occur in the lungs include weakening of the respiratory muscles as well as a decrease in lung measures of lung function such as vital capacity, which is the maximum amount of air that can be breathed out following a maximum inhalation.
Reference:
1. Janssens J, Pache J, Nicod L. Physiological changes in respiratory function associated with ageing. European Respiratory Journal. 1999;13(1):197-205. Available at: http://erj.ersjournals.com/content/13/1/197.long. Accessed October 13, 2016.
2. System E. Effects of Aging on the Respiratory System. Merck Manuals Consumer Version. 2016. Available at: https://www.merckmanuals.com/home/lung-and-airway-disorders/biology-of-the-lungs-and-airways/effects-of-aging-on-the-respiratory-system. Accessed October 13, 2016.
Reference:
1. Janssens J, Pache J, Nicod L. Physiological changes in respiratory function associated with ageing. European Respiratory Journal. 1999;13(1):197-205. Available at: http://erj.ersjournals.com/content/13/1/197.long. Accessed October 13, 2016.
2. System E. Effects of Aging on the Respiratory System. Merck Manuals Consumer Version. 2016. Available at: https://www.merckmanuals.com/home/lung-and-airway-disorders/biology-of-the-lungs-and-airways/effects-of-aging-on-the-respiratory-system. Accessed October 13, 2016.
Question 23 |
Which of the following gastroenterological changes is/are seen as body ages?
Decrease in gastric pH | |
Decrease in gastric blood flow | |
Increased gastric emptying | |
A and B |
Question 23 Explanation:
Answer B. Aging has been associated with various GI changes such as: a decrease in splanchnic blood flow, delayed gastric emptying, and an increase in gastric pH.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
Question 24 |
Which of the following physiological changes is/are seen in aging?
Decrease in dermal thickness | |
Decrease in hepatic blood flow | |
Increase in total body water | |
A and B |
Question 24 Explanation:
Answer D. Blood flow to the liver may be reduced with aging by 25-47% and dermal thickness, vascularity, and cellularity also decreases with age. There is a progressive reduction in total body water and lean body mass that occurs and which results in a relative increase in body fat.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Question 25 |
Which of the following clinical change is/are seen due to changes in drug distribution as body ages?
Increase plasma concentration of water-soluble drugs | |
Prolonged elimination half-life of fat-soluble drugs | |
Increased free fraction in plasma of high protein bound acidic drugs. | |
All of the above |
Question 25 Explanation:
Answer D. Pharmacokinetic changes in the elderly such as an increase in volume of distribution of lipid soluble drugs, results in prolonged elimination half-life of these agents. Thus, polar drugs that are mainly water-soluble tend to have smaller volumes of distribution, resulting in higher serum levels in older patients. Serum albumin (binds to acidic drugs) decrease with age, resulting in an increased free fraction in plasma of high protein bound acidic drugs.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Question 26 |
Which of the following drug concentration may increase due to reduced first-pass metabolism in elderly patients?
Morphine | |
Propranolol | |
Labetalol | |
All of the above |
Question 26 Explanation:
Answer D. Hepatic metabolism includes phase 1 reactions (oxidation, reduction and hydroxylation) and phase 2 reactions (conjugation with glucuronate, sulphate or acetate). Phase 1 reactions, are reduced during the aging process, probably due to a combination of reduced hepatic blood flow (35% reduction in hepatic blood flow in the elderly) and reduced hepatic volume. Thus, drug metabolism, particularly first-pass metabolism (e.g. propranolol, labetalol, verapamil, metoclopramide, opioids) may be considerably reduced in elderly people, which in return may increase their drug concentrations.
Reference:
1. Hughes. Prescribing for the elderly patient: why do we need to exercise caution?. British Journal of Clinical Pharmacology. 2002;46(6):531-533. doi:10.1046/j.1365-2125.1998.00842.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Reference:
1. Hughes. Prescribing for the elderly patient: why do we need to exercise caution?. British Journal of Clinical Pharmacology. 2002;46(6):531-533. doi:10.1046/j.1365-2125.1998.00842.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Question 27 |
The elimination half-life of what lipophilic drug is significantly prolonged due to increase in volume of distribution in elderly patients?
Alprazolam | |
Diazepam | |
Lorazepam | |
Triazolam |
Question 27 Explanation:
Answer B. The main effect of an increased volume of distribution is a prolongation of half-life. An increase VD and half-life have been observed for agents such as diazepam. Although, in general, the volume of distribution of most benzodiazepines tends to increase with age, for reason that are not clear, the VD of alprazolam (short half-life BZD) specifically decreases in elderly men but remains unchanged in elderly women. Triazolam is also considered to have a short half-life, compared to diazepam (highly lipophilic). Phase 2 reactions usually involve conjugation of phase 1 metabolites and appear to be unchanged by the ageing process although they may be impaired in some frail elderly people, an example of this would be lorazepam (no accumulation due to inactive metabolites.)
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Reference:
1. Mangoni AJackson S. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. British Journal of Clinical Pharmacology. 2003;57(1):6-14. doi:10.1046/j.1365-2125.2003.02007.x.
2. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-57.
Question 28 |
Which of the following water-soluble drug will require lower dosing in elderly due to decreased volume of distribution?
Lithium | |
Cimetidine | |
Digoxin | |
All of the above |
Question 28 Explanation:
Answer D. Lithium, cimetidine, and digoxin distribution in elderly is influenced by physiologic change related to body composition, particularly total body water. There is a decrease in total body water with advancing age, which results in a lower volume of water per kilogram of body weight. So the same dose of these agents in an older person would have less water for them to distribute into, resulting in a higher serum lithium concentration.
Reference:
1. Mohandas E, Rajmohan V. Lithium use in special populations. Indian Journal of Psychiatry. 2007;49(3):211. doi:10.4103/0019-5545.37325.
2. Hughes. Prescribing for the elderly patient: why do we need to exercise caution?. British Journal of Clinical Pharmacology. 2002;46(6):531-533. doi:10.1046/j.1365-2125.1998.00842.x.
Reference:
1. Mohandas E, Rajmohan V. Lithium use in special populations. Indian Journal of Psychiatry. 2007;49(3):211. doi:10.4103/0019-5545.37325.
2. Hughes. Prescribing for the elderly patient: why do we need to exercise caution?. British Journal of Clinical Pharmacology. 2002;46(6):531-533. doi:10.1046/j.1365-2125.1998.00842.x.
Question 29 |
Which of the following statement is true regarding calculating creatinine clearance in patients >65 years of age?
When serum creatinine value is less than 1mg/dl, serum creatinine should be rounded to 1 mg/dl in patients that are >65 years of age. | |
Adjusted body weight should be used in morbidly obese patients to calculate creatinine clearance. | |
Actual serum creatinine should be used to calculate creatinine clearance | |
B and C. |
Question 29 Explanation:
Answer D. An unbiased Cockcroft-Gault creatinine clearance can be calculated using actual body weight in underweight patients and ideal body weight in patients of normal weight. Using ABW(0.4) for overweight, obese, and morbidly obese patients appears to be the least biased and most accurate method for calculating their Cockcroft-Gault creatinine clearance. In addition, the common practice of rounding or replacing low Serum Creatinine values with an arbitrary value of 1.0 mg/dl for use in the CG equation should be avoided. Rounding S(c) (r) in patients with low S(c) (r) did not improve accuracy or bias of the creatinine clearance calculations.
Reference:
1. Dowling T, Wang E, Ferrucci L, Sorkin J. Glomerular Filtration Rate Equations Overestimate Creatinine Clearance in Older Individuals Enrolled in the Baltimore Longitudinal Study on Aging: Impact on Renal Drug Dosing. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2013;33(9):912-921. doi:10.1002/phar.1282.
2. Winter MA e. Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22576791. Accessed October 13, 2016.
Reference:
1. Dowling T, Wang E, Ferrucci L, Sorkin J. Glomerular Filtration Rate Equations Overestimate Creatinine Clearance in Older Individuals Enrolled in the Baltimore Longitudinal Study on Aging: Impact on Renal Drug Dosing. Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy. 2013;33(9):912-921. doi:10.1002/phar.1282.
2. Winter MA e. Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. - PubMed - NCBI. Ncbinlmnihgov. 2016. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22576791. Accessed October 13, 2016.
Once you are finished, click the button below. Any items you have not completed will be marked incorrect.
There are 29 questions to complete.
|
List |

Comments are closed.